

Pre-operative MRI Radiomics for the Prediction of Progression and Recurrence in Meningiomas
- PMID: 34054688
- PMCID: PMC8160291
- DOI: 10.3389/fneur.2021.636235
Pre-operative MRI Radiomics for the Prediction of Progression and Recurrence in Meningiomas
Abstract
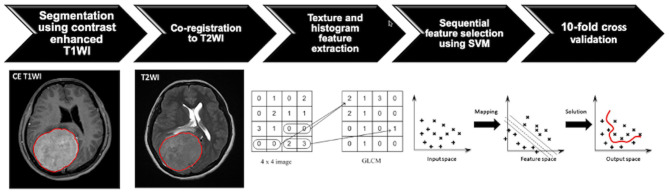
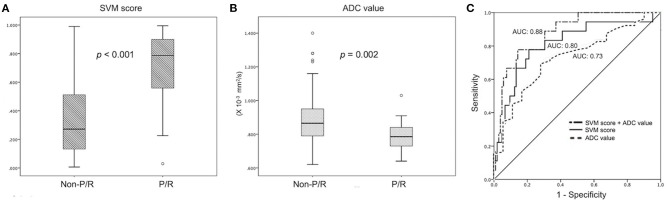
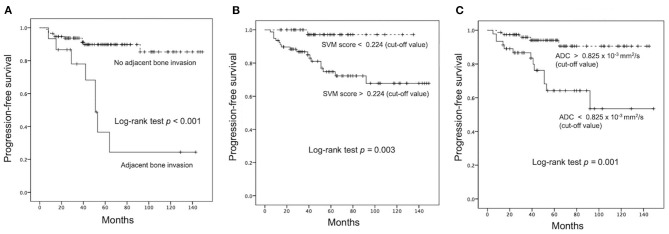
Objectives: A subset of meningiomas may show progression/recurrence (P/R) after surgical resection. This study applied pre-operative MR radiomics based on support vector machine (SVM) to predict P/R in meningiomas. Methods: From January 2007 to January 2018, 128 patients with pathologically confirmed WHO grade I meningiomas were included. Only patients who had undergone pre-operative MRIs and post-operative follow-up MRIs for more than 1 year were studied. Pre-operative T2WI and contrast-enhanced T1WI were analyzed. On each set of images, 32 first-order features and 75 textural features were extracted. The SVM classifier was utilized to evaluate the significance of extracted features, and the most significant four features were selected to calculate SVM score for each patient. Results: Gross total resection (Simpson grades I-III) was performed in 93 (93/128, 72.7%) patients, and 19 (19/128, 14.8%) patients had P/R after surgery. Subtotal tumor resection, bone invasion, low apparent diffusion coefficient (ADC) value, and high SVM score were more frequently encountered in the P/R group (p < 0.05). In multivariate Cox hazards analysis, bone invasion, ADC value, and SVM score were high-risk factors for P/R (p < 0.05) with hazard ratios of 7.31, 4.67, and 8.13, respectively. Using the SVM score, an AUC of 0.80 with optimal cutoff value of 0.224 was obtained for predicting P/R. Patients with higher SVM scores were associated with shorter progression-free survival (p = 0.003). Conclusions: Our preliminary results showed that pre-operative MR radiomic features may have the potential to offer valuable information in treatment planning for meningiomas.
Keywords: magnetic resonance imaging; meningioma; progression; radiomics; recurrence; support vector machine.
Copyright © 2021 Ko, Zhang, Chen, Chang, Chen, Lim, Wu and Su.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Maillo A, Orfao A, Espinosa AB, Sayagues JM, Merino M, Sousa P, et al. . Early recurrences in histologically benign/grade i meningiomas are associated with large tumors and coexistence of monosomy 14 and del(1p36) in the ancestral tumor cell clone. Neuro Oncol. (2007) 9:438–6. 10.1215/15228517-2007-026 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials