

Antigen-Specific Regulatory T Cell Therapy in Autoimmune Diseases and Transplantation
- PMID: 34054826
- PMCID: PMC8160309
- DOI: 10.3389/fimmu.2021.661875
Antigen-Specific Regulatory T Cell Therapy in Autoimmune Diseases and Transplantation
Abstract
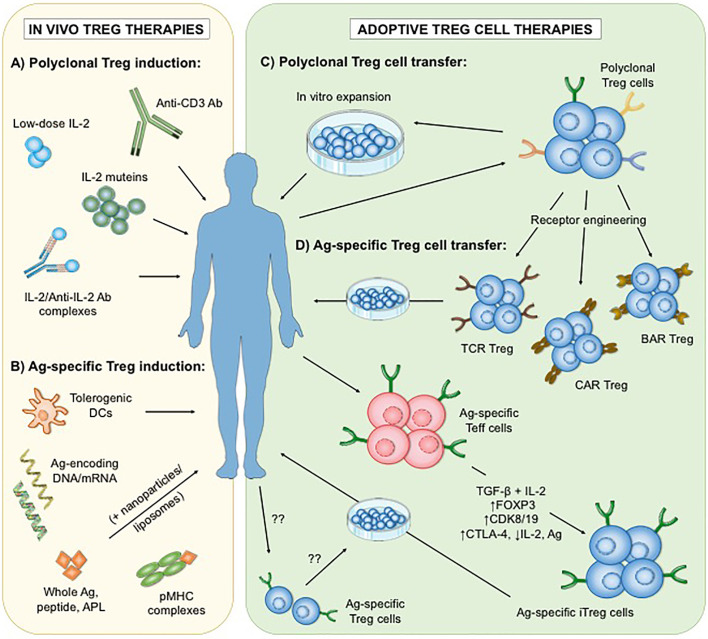
Regulatory T (Treg) cells are a heterogenous population of immunosuppressive T cells whose therapeutic potential for the treatment of autoimmune diseases and graft rejection is currently being explored. While clinical trial results thus far support the safety and efficacy of adoptive therapies using polyclonal Treg cells, some studies suggest that antigen-specific Treg cells are more potent in regulating and improving immune tolerance in a disease-specific manner. Hence, several approaches to generate and/or expand antigen-specific Treg cells in vitro or in vivo are currently under investigation. However, antigen-specific Treg cell therapies face additional challenges that require further consideration, including the identification of disease-relevant antigens as well as the in vivo stability and migratory behavior of Treg cells following transfer. In this review, we discuss these approaches and the potential limitations and describe prospective strategies to enhance the efficacy of antigen-specific Treg cell treatments in autoimmunity and transplantation.
Keywords: Tregs; antigen-specific Tregs; autoimmune disease (AD); regulatory T cells; therapy; transplantation.
Copyright © 2021 Selck and Dominguez-Villar.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Treg cell-based therapies: challenges and perspectives.Nat Rev Immunol. 2020 Mar;20(3):158-172. doi: 10.1038/s41577-019-0232-6. Epub 2019 Dec 6. Nat Rev Immunol. 2020. PMID: 31811270 Free PMC article. Review.
-
The Next Frontier of Regulatory T Cells: Promising Immunotherapy for Autoimmune Diseases and Organ Transplantations.Front Immunol. 2020 Sep 23;11:565518. doi: 10.3389/fimmu.2020.565518. eCollection 2020. Front Immunol. 2020. PMID: 33072105 Free PMC article. Review.
-
Regulating the regulators: Is introduction of an antigen-specific approach in regulatory T cells the next step to treat autoimmunity?Cell Immunol. 2020 Dec;358:104236. doi: 10.1016/j.cellimm.2020.104236. Epub 2020 Oct 13. Cell Immunol. 2020. PMID: 33137651 Review.
-
Treg Enhancing Therapies to Treat Autoimmune Diseases.Int J Mol Sci. 2020 Sep 23;21(19):7015. doi: 10.3390/ijms21197015. Int J Mol Sci. 2020. PMID: 32977677 Free PMC article. Review.
-
Manipulating regulatory T cells: a promising strategy to treat autoimmunity.Immunotherapy. 2015;7(11):1201-11. doi: 10.2217/imt.15.79. Epub 2015 Nov 16. Immunotherapy. 2015. PMID: 26568117 Free PMC article. Review.
Cited by
-
Identification of Liver Immune Microenvironment-Related Hub Genes in Liver of Biliary Atresia.Front Pediatr. 2022 Jan 17;9:786422. doi: 10.3389/fped.2021.786422. eCollection 2021. Front Pediatr. 2022. PMID: 35111704 Free PMC article.
-
Bone Morphogenetic Proteins Shape Treg Cells.Front Immunol. 2022 Mar 28;13:865546. doi: 10.3389/fimmu.2022.865546. eCollection 2022. Front Immunol. 2022. PMID: 35418975 Free PMC article. Review.
-
Revisiting regulatory T cells as modulators of innate immune response and inflammatory diseases.Front Immunol. 2023 Oct 20;14:1287465. doi: 10.3389/fimmu.2023.1287465. eCollection 2023. Front Immunol. 2023. PMID: 37928540 Free PMC article. Review.
-
Translation of cell therapies to treat autoimmune disorders.Adv Drug Deliv Rev. 2024 Feb;205:115161. doi: 10.1016/j.addr.2023.115161. Epub 2023 Dec 22. Adv Drug Deliv Rev. 2024. PMID: 38142739 Free PMC article. Review.
-
Dual neutralization of TGF-β and IL-21 regulates Th17/Treg balance by suppressing inflammatory signalling in the splenic lymphocytes of Staphylococcus aureus infection-induced septic arthritic mice.Immunol Res. 2025 Jan 20;73(1):38. doi: 10.1007/s12026-024-09586-2. Immunol Res. 2025. PMID: 39831928
References
-
- Coombes JL, Siddiqui KR, Arancibia-Carcamo CV, Hall J, Sun CM, Belkaid Y, et al. . A Functionally Specialized Population of Mucosal CD103+ Dcs Induces Foxp3+ Regulatory T Cells Via a TGF-beta and Retinoic Acid-Dependent Mechanism. J Exp Med (2007) 204:1757–64. 10.1084/jem.20070590 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical