

Use of B-Type Natriuretic Peptide (BNP) and N-Terminal proBNP (NT-proBNP) as Diagnostic Tests in Adults With Suspected Heart Failure: A Health Technology Assessment
- PMID: 34055110
- PMCID: PMC8129637
Use of B-Type Natriuretic Peptide (BNP) and N-Terminal proBNP (NT-proBNP) as Diagnostic Tests in Adults With Suspected Heart Failure: A Health Technology Assessment
Abstract
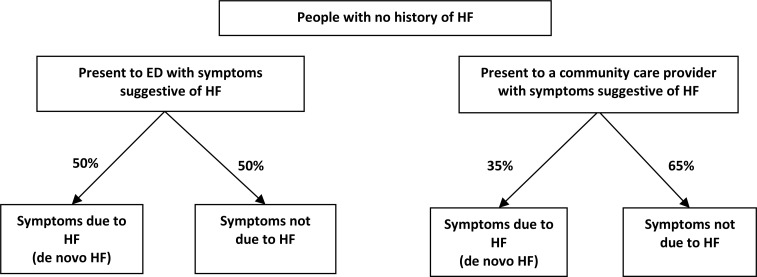
Background: Heart failure is a complex clinical syndrome that usually presents with breathlessness, leg edema, and fatigue. Clinically measurable natriuretic neurohormones such as B-type natriuretic peptide (BNP) and N-terminal proBNP (NT-proBNP) are elevated in people with heart failure. We conducted a health technology assessment of BNP and NT-proBNP tests for people with suspected heart failure, which included an evaluation of diagnostic accuracy, clinical impact, cost-effectiveness, the budget impact of publicly funding BNP and NT-proBNP tests, and patient preferences and values.
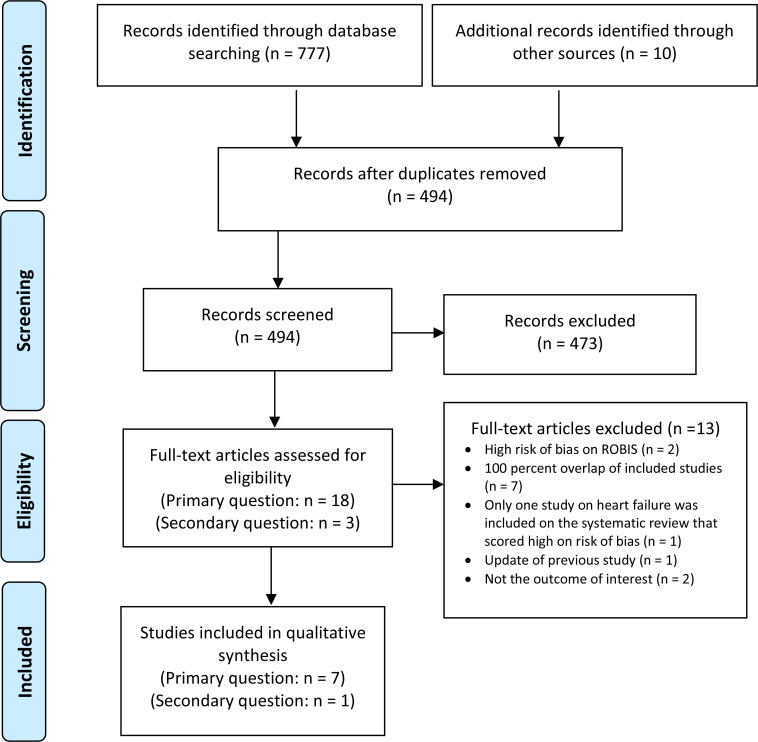
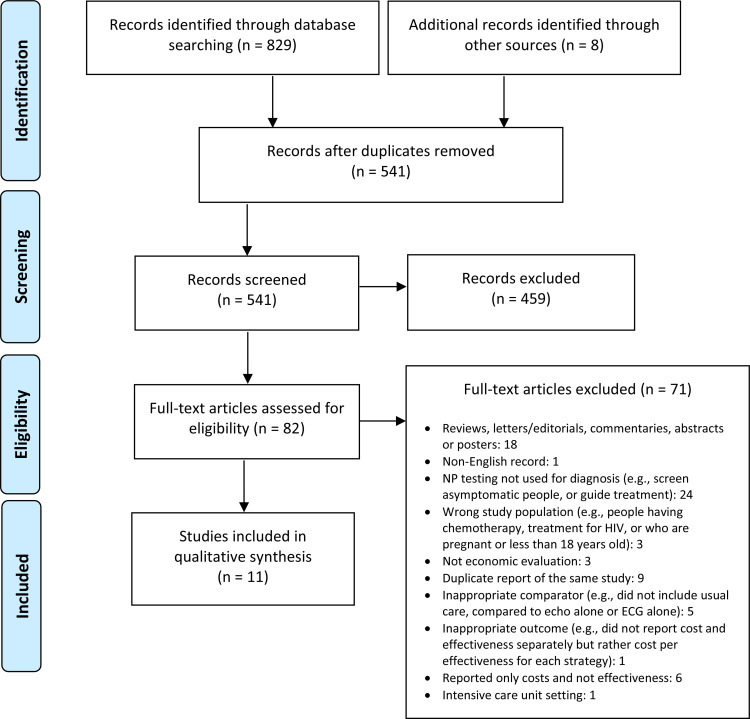
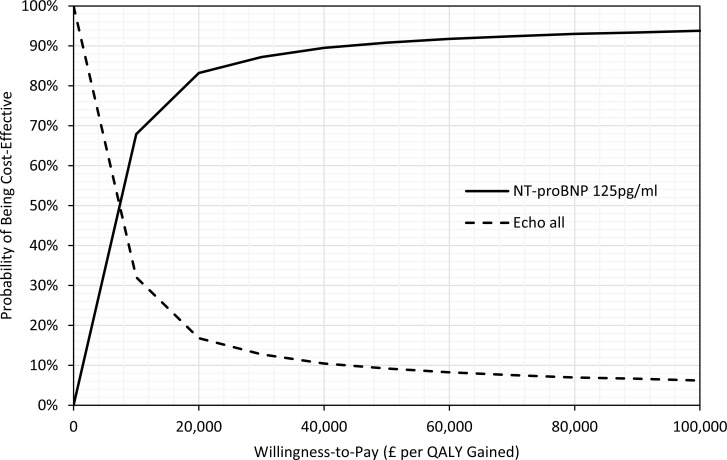
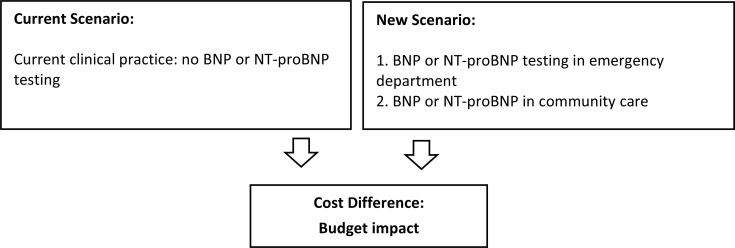
Methods: We performed a literature search of previously published systematic reviews of the clinical evidence. We conducted an overview of reviews and included only reviews with a low risk of bias as assessed using the Risk of Bias in Systematic Reviews tool (ROBIS). We excluded any reviews where we found 100% overlap of included primary studies and selected systematic reviews or health technology assessments published after 2006 for inclusion.We performed an economic literature review of BNP and NT-proBNP testing in people with suspected heart failure. Medical and health economic databases were searched from database inception until July 25, 2019. Next, we assessed the cost-effectiveness of BNP and NT-proBNP based on the published economic literature. We transferred the cost-effectiveness results of two applicable, recent economic evaluations from the National Institute for Health and Care Excellence (NICE) to the Ontario setting in lieu of conducting de novo primary economic evaluations. We also estimated the budget impact of publicly funding BNP and NT-proBNP tests in people with suspected heart failure in Ontario over the next 5 years.To contextualize the potential value of BNP and NT-proBNP testing, we spoke with people with suspected heart failure.
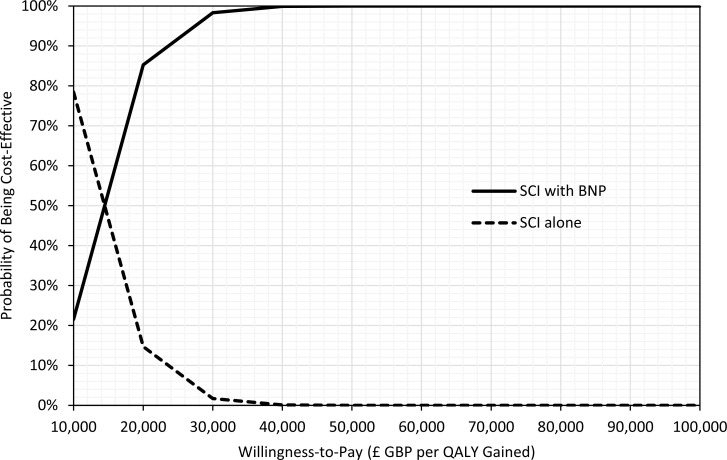
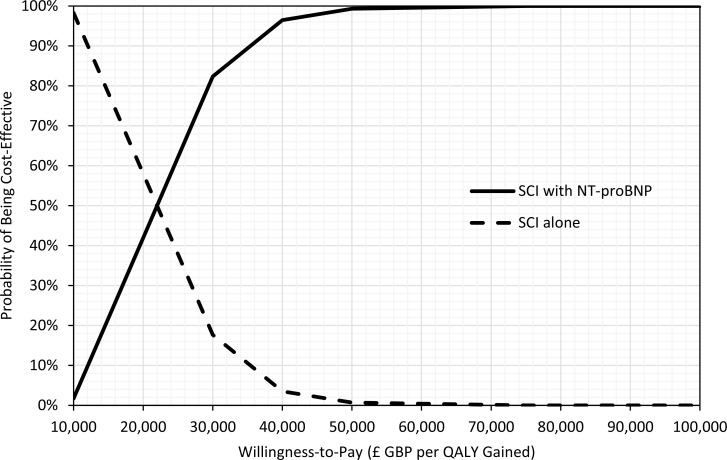
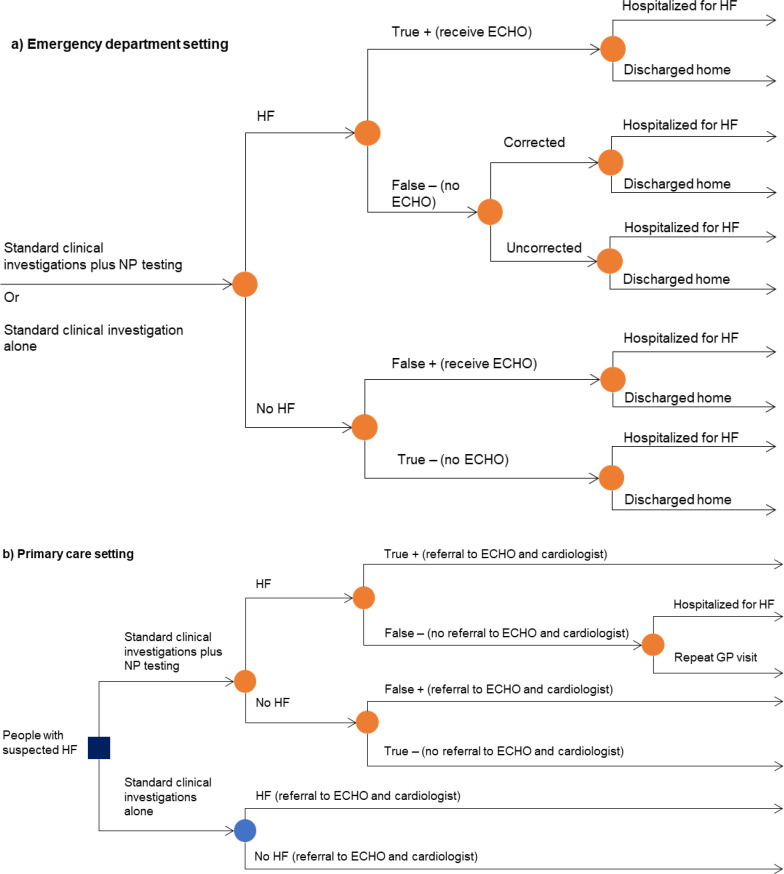
Results: We included eight systematic reviews in the clinical evidence review. B-type natriuretic peptides and NT-proBNP had a high pooled sensitivity (80% to 94% and 86% to 96%, respectively; strength of evidence: high) and a low pooled negative likelihood ratio (0.08-0.30 and 0.09-0.23, respectively; strength of evidence: not reported) within varying thresholds or cut points and settings, as reported in seven systematic reviews. In one systematic review, when BNP or NT-proBNP was used in the diagnosis of heart failure in the emergency department (ED), there was a decrease in the mean length of hospital stay (-1.22 days; confidence interval [CI] -2.31 to -0.14; Grading of Recommendations Assessment, Development, and Evaluation [GRADE] Working Group criteria: Moderate). B-type natriuretic peptide testing did not reduce hospital admission rates (odds ratio [OR]: 0.82; CI: 0.67-1.01; GRADE: Moderate), 30-day hospital readmission rates (OR: 0.88; CI: 0.64-1,20; GRADE: Moderate), or hospital mortality rates (OR: 0.96; CI: 0.65-1.41; GRADE: Moderate). No systematic review was identified that addressed the impact on clinical outcomes of BNP use in the community setting.Our economic literature review found a total of 12 studies evaluating the cost-effectiveness of BNP or NT-proBNP testing in patients with suspected heart failure. The studies suggested that BNP or NT-proBNP tests, when used in addition to standard clinical investigations, were either dominant (less costly and more effective) or cost-effective across different countries (including Canada) and settings.Two economic evaluations conducted by NICE were considered applicable to our research question and of high methodological quality. Based on the transferred results from the two NICE economic evaluations, we concluded that BNP and NT-proBNP were highly likely to be cost-effective in Ontario in the ED setting, and NT-proBNP was highly likely to be cost-effective in the community care setting.Our budget impact analysis estimated that over the next 5 years, publicly funding BNP and NT-proBNP tests would result in an additional cost of $38 million in the ED (at a cost of $75 per test) and a cost savings of $20 million in community care (at a cost of $28 per test).We received strong support from interview participants about BNP or NT-proBNP diagnostic testing. The main reason was the perceived potential benefit of receiving a speedier diagnosis. The overall process, from diagnosis to treatment, is a substantial emotional burden for patients and caregivers, and for those living further away from secondary or tertiary care settings. An earlier diagnosis could allow patients to receive treatment at a hospital better equipped to manage their potentially fatal symptoms and conditions.
Conclusions: B-type natriuretic peptide and NT-proBNP tests have high sensitivity and low negative likelihood ratio, suggesting that concentrations of either natriuretic peptides within the appropriate cut points can rule out the presence of heart failure with a high degree of confidence. Additionally, BNP or NT-proBNP testing along with usual care in an ED setting likely can reduce the length of hospital stay by at least 1 day but likely results in little to no difference in hospital mortality, 30-day readmission, or admission rates to hospital.Based on the published economic literature, we expected BNP or NT-proBNP tests used in addition to standard clinical investigations to be cost-effective as a rule-out test in patients with suspected heart failure in Ontario. If BNP and NT-proBNP tests are publicly funded in Ontario, we estimated that there would be additional costs in the ED setting (due to increased detection of heart failure) and savings in community care (due to reduced referrals to echocardiography and cardiologists).People we interviewed gave BNP and NT-proBNP testing strong support, citing the perceived benefits of quicker, more accurate diagnoses that could reduce misdiagnoses, stress, and the burden on patients and caregivers.
Copyright © Queen's Printer for Ontario, 2021.
Figures
Similar articles
-
Multi-gene Pharmacogenomic Testing That Includes Decision-Support Tools to Guide Medication Selection for Major Depression: A Health Technology Assessment.Ont Health Technol Assess Ser. 2021 Aug 12;21(13):1-214. eCollection 2021. Ont Health Technol Assess Ser. 2021. PMID: 34484487 Free PMC article.
-
Level 2 Polysomnography for the Diagnosis of Sleep Disorders: A Health Technology Assessment.Ont Health Technol Assess Ser. 2024 Aug 20;24(7):1-157. eCollection 2024. Ont Health Technol Assess Ser. 2024. PMID: 39372311 Free PMC article.
-
Interferon-Gamma Release Assay Testing for Latent Tuberculosis Infection: A Health Technology Assessment.Ont Health Technol Assess Ser. 2024 Dec 12;24(11):1-183. eCollection 2024. Ont Health Technol Assess Ser. 2024. PMID: 39911267 Free PMC article.
-
Placental Growth Factor (PlGF)- Based Biomarker Testing to Help Diagnose Pre-eclampsia in People With Suspected Pre-eclampsia: A Health Technology Assessment.Ont Health Technol Assess Ser. 2023 May 17;23(3):1-146. eCollection 2023. Ont Health Technol Assess Ser. 2023. PMID: 37284279 Free PMC article.
-
Supplemental Screening as an Adjunct to Mammography for Breast Cancer Screening in People With Dense Breasts: A Health Technology Assessment.Ont Health Technol Assess Ser. 2023 Dec 19;23(9):1-293. eCollection 2023. Ont Health Technol Assess Ser. 2023. PMID: 39364436 Free PMC article.
Cited by
-
Early Diagnosis of Chemotherapy-Linked Cardiotoxicity in Breast Cancer Patients Using Conventional Biomarker Panel: A Prospective Study Protocol.Diagnostics (Basel). 2022 Nov 6;12(11):2714. doi: 10.3390/diagnostics12112714. Diagnostics (Basel). 2022. PMID: 36359556 Free PMC article.
-
Clinical practice guidelines for diagnostic and treatment of the chronic heart failure.Arch Cardiol Mex. 2024;94(Supl 1):1-74. doi: 10.24875/ACM.M24000095. Arch Cardiol Mex. 2024. PMID: 38648647 Free PMC article. English.
-
Low Socioeconomic Status Is Associated with Reduced Access to Natriuretic Peptide Testing in the Outpatient Setting: A Population-based Evaluation.CJC Open. 2025 Jan 7;7(4):390-401. doi: 10.1016/j.cjco.2025.01.002. eCollection 2025 Apr. CJC Open. 2025. PMID: 40433145 Free PMC article.
-
The Use of Brain Natriuretic Peptide in the Evaluation of Heart Failure in Geriatric Patients.Diagnostics (Basel). 2023 Apr 23;13(9):1512. doi: 10.3390/diagnostics13091512. Diagnostics (Basel). 2023. PMID: 37174904 Free PMC article. Review.
-
The relationship between peripheral blood soluble ST2, BNP levels, cardiac function, and prognosis in patients with heart failure.Am J Transl Res. 2023 Apr 15;15(4):2878-2884. eCollection 2023. Am J Transl Res. 2023. PMID: 37193147 Free PMC article.
References
-
- Canadian Cardiovascular Society. Pocket guides [Internet]. Ottawa (ON): Canadian Cardiovascular Society; c2020. Available from: https://www.ccs.ca/en/resources/pocket-guides
-
- Ezekowitz JA, O'Meara E, McDonald MA, Abrams H, Chan M, Ducharme A, et al. 2017 comprehensive update of the Canadian Cardiovascular Society guidelines for the management of heart failure. Can J Cardiol. 2017;33(11):1342–433. - PubMed
-
- Heart and Stroke Foundation. 2016 report on the health of Canadians: the burden of heart failure [Internet]. Ottawa (ON): Heart & Stroke; 2016. Available from: https://www.heartandstroke.ca/-/media/pdf-files/canada/2017-heart-month/...
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. Corrigendum to: ‘2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure’. Eur Heart J. 2018;39(14):1206. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18(8):891–975. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials