

Acute syndesmotic injuries in ankle fractures: From diagnosis to treatment and current concepts
- PMID: 34055585
- PMCID: PMC8152437
- DOI: 10.5312/wjo.v12.i5.270
Acute syndesmotic injuries in ankle fractures: From diagnosis to treatment and current concepts
Abstract
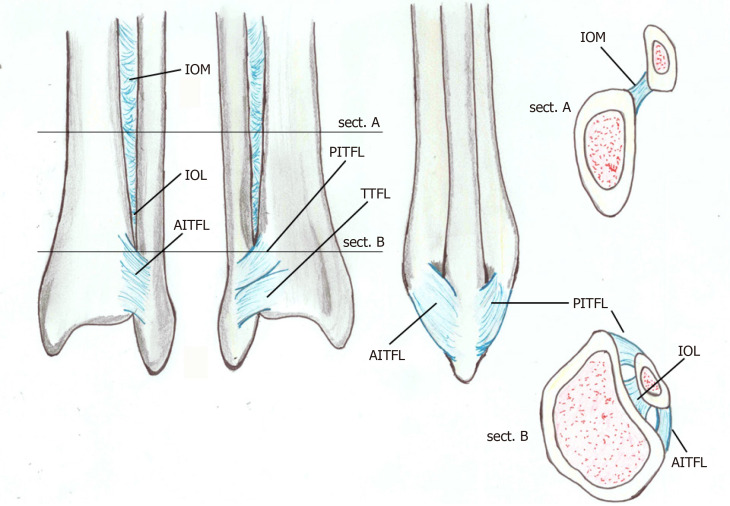
A stable and precise articulation of the distal tibiofibular syndesmosis maintains the tibiofibular relationship, and it is essential for normal motion of the ankle joint. The disruption of this joint is frequently accompanied by rotational ankle fracture, such as pronation-external rotation, and rarely occurs without ankle fracture. The diagnosis is not simple, and ideal management of the various presentations of syndesmotic injury remains controversial to this day. Anatomical restoration and stabilization of the disrupted tibiofibular syndesmosis is essential to improve functional outcomes. In such an injury, including inadequately treated, misdiagnosed and correctly diagnosed cases, a chronic pattern characterized by persistent ankle pain, function disability and early osteoarthritis can result. This paper reviews anatomical and biomechanical characteristics of this syndesmosis, the mechanism of its acute injury associated to fractures, radiological and arthroscopic diagnosis and surgical treatment.
Keywords: Ankle; Distal tibiofibular joint; Fracture; Injury; Syndesmosis; Trauma.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no conflict of interests for this article.
Figures



Similar articles
-
Management of chronic disruption of the distal tibiofibular syndesmosis.World J Orthop. 2011 Jan 18;2(1):1-6. doi: 10.5312/wjo.v2.i1.1. World J Orthop. 2011. PMID: 22474625 Free PMC article.
-
[TREATMENT OF PRONATION EXTERNAL ROTATION ANKLE FRACTURE COMBINED WITH SEPARATION OF DISTAL TIBIOFIBULAR SYNDESMOSIS].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2016 Sep 8;30(9):1081-1084. doi: 10.7507/1002-1892.20160220. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2016. PMID: 29786359 Chinese.
-
[Injuries of the inferior tibiofibular syndesmosis].Unfallchirurg. 2000 Jul;103(7):520-32. Unfallchirurg. 2000. PMID: 10969538 Review. German.
-
Distal Tibiofibular Syndesmosis: Anatomy, Biomechanics, Injury and Management.Open Orthop J. 2017 Jul 31;11:670-677. doi: 10.2174/1874325001711010670. eCollection 2017. Open Orthop J. 2017. PMID: 29081864 Free PMC article. Review.
-
Ankle fractures involving the fibula proximal to the distal tibiofibular syndesmosis.Foot Ankle Int. 1997 Aug;18(8):513-21. doi: 10.1177/107110079701800811. Foot Ankle Int. 1997. PMID: 9278748 Review.
Cited by
-
Direct versus indirect posterior malleolar fixation in the treatment of trimalleolar ankle fractures: Is there a difference in outcomes?OTA Int. 2022 Oct 6;5(4):e219. doi: 10.1097/OI9.0000000000000219. eCollection 2022 Dec. OTA Int. 2022. PMID: 36569113 Free PMC article.
-
Quadrimalleolar ankle fracture with syndesmosis disruption-a minimally invasive approach with arthroscopic repair of the anterior-inferior tibiofibular ligament (AITFL); a case report.Trauma Case Rep. 2025 Apr 18;57:101173. doi: 10.1016/j.tcr.2025.101173. eCollection 2025 May. Trauma Case Rep. 2025. PMID: 40330843 Free PMC article.
-
A 10-Year Follow-Up of Ankle Syndesmotic Injuries: Prospective Comparison of Knotless Suture-Button Fixation and Syndesmotic Screw Fixation.J Clin Med. 2022 Apr 30;11(9):2524. doi: 10.3390/jcm11092524. J Clin Med. 2022. PMID: 35566650 Free PMC article.
-
Prevalence and Characteristics of Patients Requiring Surgical Reinterventions for Ankle Fractures.J Clin Med. 2023 Sep 8;12(18):5843. doi: 10.3390/jcm12185843. J Clin Med. 2023. PMID: 37762784 Free PMC article.
-
The Radiological Anatomy of the Distal Tibiofibular Joint: A Retrospective Computed Tomography Study.Cureus. 2024 Feb 4;16(2):e53540. doi: 10.7759/cureus.53540. eCollection 2024 Feb. Cureus. 2024. PMID: 38318279 Free PMC article.
References
-
- Kocadal O, Yucel M, Pepe M, Aksahin E, Aktekin CN. Evaluation of Reduction Accuracy of Suture-Button and Screw Fixation Techniques for Syndesmotic Injuries. Foot Ankle Int . 2016;37:1317–1325. - PubMed
-
- Lubberts B, Guss D, Vopat BG, Johnson AH, van Dijk CN, Lee H, DiGiovanni CW. The arthroscopic syndesmotic assessment tool can differentiate between stable and unstable ankle syndesmoses. Knee Surg Sports Traumatol Arthrosc . 2020;28:193–201. - PubMed
-
- Gan K, Xu D, Hu K, Wu W, Shen Y. Dynamic fixation is superior in terms of clinical outcomes to static fixation in managing distal tibiofibular syndesmosis injury. Knee Surg Sports Traumatol Arthrosc . 2020;28:270–280. - PubMed
-
- Brosky T, Nyland J, Nitz A, Caborn DN. The ankle ligaments: consideration of syndesmotic injury and implications for rehabilitation. J Orthop Sports Phys Ther . 1995;21:197–205. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
