

Arthroscopic "Debridement and Implant Retention" With Local Administration of Exebacase (Lysin CF-301) Followed by Suppressive Tedizolid as Salvage Therapy in Elderly Patients for Relapsing Multidrug-Resistant S. epidermidis Prosthetic Knee Infection
- PMID: 34055817
- PMCID: PMC8163228
- DOI: 10.3389/fmed.2021.550853
Arthroscopic "Debridement and Implant Retention" With Local Administration of Exebacase (Lysin CF-301) Followed by Suppressive Tedizolid as Salvage Therapy in Elderly Patients for Relapsing Multidrug-Resistant S. epidermidis Prosthetic Knee Infection
Abstract
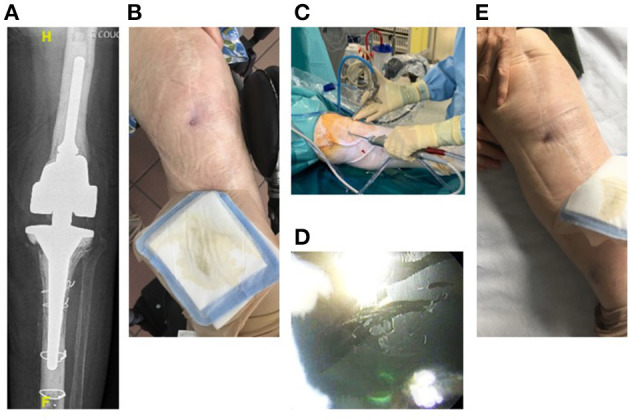
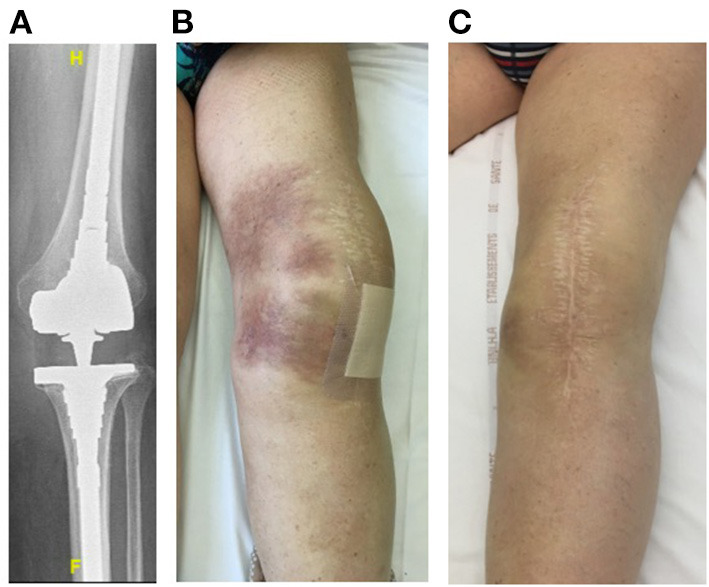
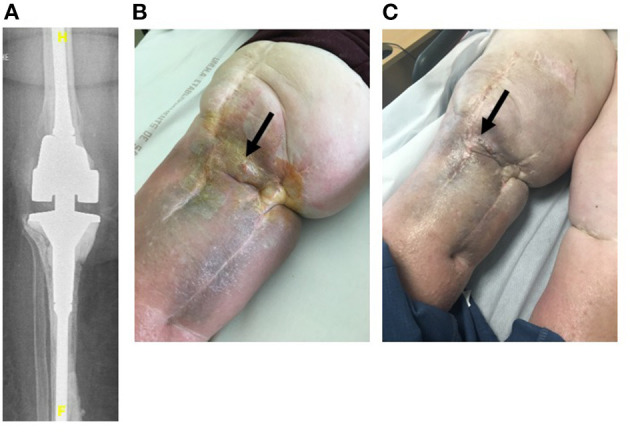
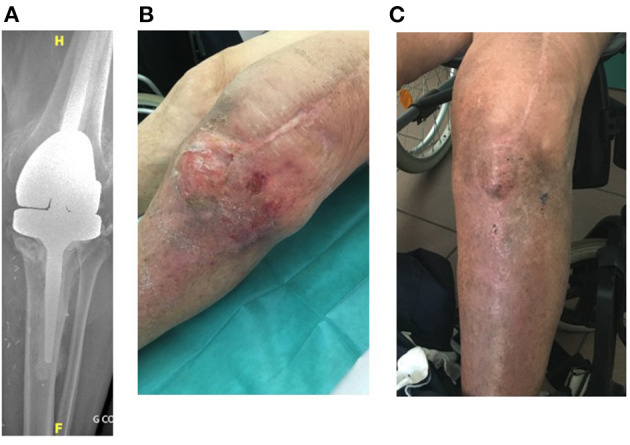
Exebacase, a recombinantly produced lysin has recently (i) reported proof-of-concept data from a phase II study in S. aureus bacteremia and (ii) demonstrated antibiofilm activity in vitro against S. epidermidis. In patients with relapsing multidrug-resistant (MDR) S. epidermidis prosthetic knee infection (PKI), the only surgical option is prosthesis exchange. In elderly patients who have undergone several revisions, prosthesis explantation could be associated with definitive loss of function and mortality. In our BJI reference regional center, arthroscopic debridement and implant retention with local administration of exebacase (LysinDAIR) followed by suppressive tedizolid as salvage therapy is proposed for elderly patients with recurrent MDR S. epidermidis PKI with no therapeutic option or therapeutic dead end (for whom revision or transfemoral amputation is not feasible and no other oral option is available). Each use was decided in agreement with the French health authority and in accordance with the local ethics committee. A written consent was obtained for each patient. Exebacase (75 mg/mL; 30 mL) was administered directly into the joint during arthroscopy. Four patients (79-89 years old) were treated with the LysinDAIR procedure. All had several previous prosthetic knee revisions without prosthesis loosening. Three had relapsing PKI despite suppressive antibiotics following open DAIR. Two had clinical signs of septic arthritis; the two others had sinus tract. After the LysinDAIR procedure, no adverse events occurred during arthroscopy; all patients received daptomycin 8 mg/kg and linezolid 600 mg bid (4-6 weeks) as primary therapy, followed by tedizolid 200 mg/day as suppressive therapy. At 6 months, recurrence of the sinus tract occurred in the two patients with sinus tract at baseline. After >1 year follow up, the clinical outcome was favorable in the last two patients with total disappearance of clinical signs of septic arthritis even if microbiological persistence was detected in one of them. Exebacase has the potential to be used in patients with staphylococci PKI during arthroscopic DAIR as salvage therapy to improve the efficacy of suppressive antibiotics and to prevent major loss of function.
Keywords: S. epidermidis; bacteriophage; lysin; prosthetic-joint infection; staphylococci; tedizolid.
Copyright © 2021 Ferry, Batailler, Souche, Cassino, Chidiac, Perpoint, le Corvaisier, Josse, Gaillard, Roger, Kolenda, Lustig, Laurent and the Lyon BJI Study Group.
Conflict of interest statement
CCa is employed by the company Contrafect. TF received honorarium as speaker from Contrafect to present these results to the company members. The Hospices Civils de Lyon - Institut des Agents Infectieux received financial support for a research project aimed at evaluating in vitro Lysin CF-301 activity on a collection of clinical strains. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Phage Therapy as Adjuvant to Conservative Surgery and Antibiotics to Salvage Patients With Relapsing S. aureus Prosthetic Knee Infection.Front Med (Lausanne). 2020 Nov 16;7:570572. doi: 10.3389/fmed.2020.570572. eCollection 2020. Front Med (Lausanne). 2020. PMID: 33304911 Free PMC article.
-
Salvage Debridement, Antibiotics and Implant Retention ("DAIR") With Local Injection of a Selected Cocktail of Bacteriophages: Is It an Option for an Elderly Patient With Relapsing Staphylococcus aureus Prosthetic-Joint Infection?Open Forum Infect Dis. 2018 Oct 24;5(11):ofy269. doi: 10.1093/ofid/ofy269. eCollection 2018 Nov. Open Forum Infect Dis. 2018. PMID: 30474047 Free PMC article.
-
Case Report: Arthroscopic "Debridement Antibiotics and Implant Retention" With Local Injection of Personalized Phage Therapy to Salvage a Relapsing Pseudomonas Aeruginosa Prosthetic Knee Infection.Front Med (Lausanne). 2021 May 5;8:569159. doi: 10.3389/fmed.2021.569159. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34026768 Free PMC article.
-
Debridement, antibiotics, and implant retention for periprosthetic knee infections: a pooling analysis of 1266 cases.J Orthop Surg Res. 2019 Nov 12;14(1):358. doi: 10.1186/s13018-019-1378-4. J Orthop Surg Res. 2019. PMID: 31718644 Free PMC article.
-
The Role of Long-Term Antibiotic Suppression in the Management of Peri-Prosthetic Joint Infections Treated With Debridement, Antibiotics, and Implant Retention: A Systematic Review.J Arthroplasty. 2020 Apr;35(4):1154-1160. doi: 10.1016/j.arth.2019.11.026. Epub 2019 Dec 9. J Arthroplasty. 2020. PMID: 31955984
Cited by
-
Local Antibiotic Delivery Options in Prosthetic Joint Infection.Antibiotics (Basel). 2023 Apr 14;12(4):752. doi: 10.3390/antibiotics12040752. Antibiotics (Basel). 2023. PMID: 37107114 Free PMC article. Review.
-
Bacteriophage therapy in musculoskeletal infections: from basic science to clinical application.EFORT Open Rev. 2024 May 10;9(5):339-348. doi: 10.1530/EOR-24-0042. EFORT Open Rev. 2024. PMID: 38726986 Free PMC article. Review.
-
Exebacase: A Novel Approach to the Treatment of Staphylococcal Infections.Drugs R D. 2022 Jun;22(2):113-117. doi: 10.1007/s40268-022-00383-6. Epub 2022 Feb 17. Drugs R D. 2022. PMID: 35175568 Free PMC article. Review.
-
Severe Optic Neuropathy Induced by Very Prolonged Tedizolid as Suppressive Therapy: Description of a Case Report and Implication for Better Assessment.Open Forum Infect Dis. 2024 Sep 24;11(9):ofae517. doi: 10.1093/ofid/ofae517. eCollection 2024 Sep. Open Forum Infect Dis. 2024. PMID: 39329109 Free PMC article.
-
Past and Future of Phage Therapy and Phage-Derived Proteins in Patients with Bone and Joint Infection.Viruses. 2021 Dec 2;13(12):2414. doi: 10.3390/v13122414. Viruses. 2021. PMID: 34960683 Free PMC article. Review.
References
-
- Société de Pathologie Infectieuse de Langue Française (SPILF), Collège des Universitaires de Maladies Infectieuses et Tropicales (CMIT), Groupe de Pathologie Infectieuse Pédiatrique (GPIP), Société Française d'Anesthésie et de Réanimation (SFAR), Société Française de Chirurgie Orthopédique et Traumatologique (SOFCOT), Société Française d'Hygiène Hospitalière (SFHH) et al. . Recommendations for bone and joint prosthetic device infections in clinical practice (prosthesis, implants, osteosynthesis). Med Mal Infect. (2010) 40:185–211. 10.1016/j.medmal.2009.12.009 - DOI - PubMed
-
- Ariza J, Cobo J, Baraia-Etxaburu J, Benito N, Bori G, Cabo J, et al. . Executive summary of management of prosthetic joint infections. Clinical practice guidelines by the Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC). Enferm Infecc Microbiol Clin. (2017) 35:189–95. 10.1016/j.eimce.2017.02.013 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources