Accuracy of commercial intraoral scanners
- PMID: 34056032
- PMCID: PMC8142031
- DOI: 10.1117/1.JMI.8.3.035501
Accuracy of commercial intraoral scanners
Abstract
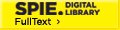
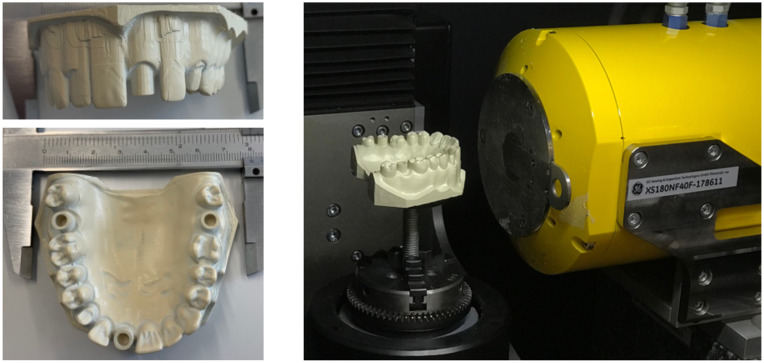
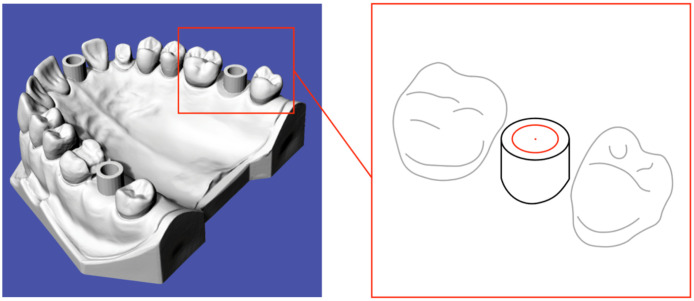
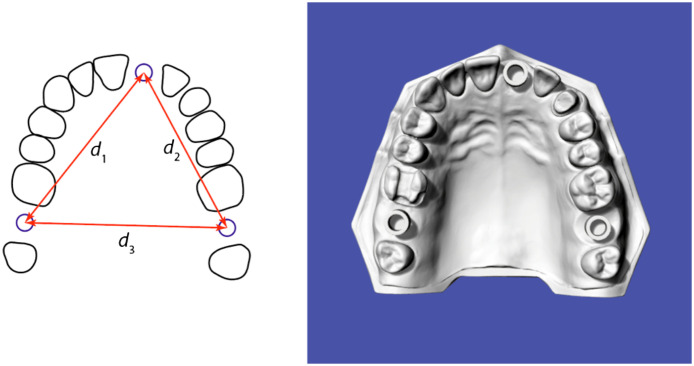
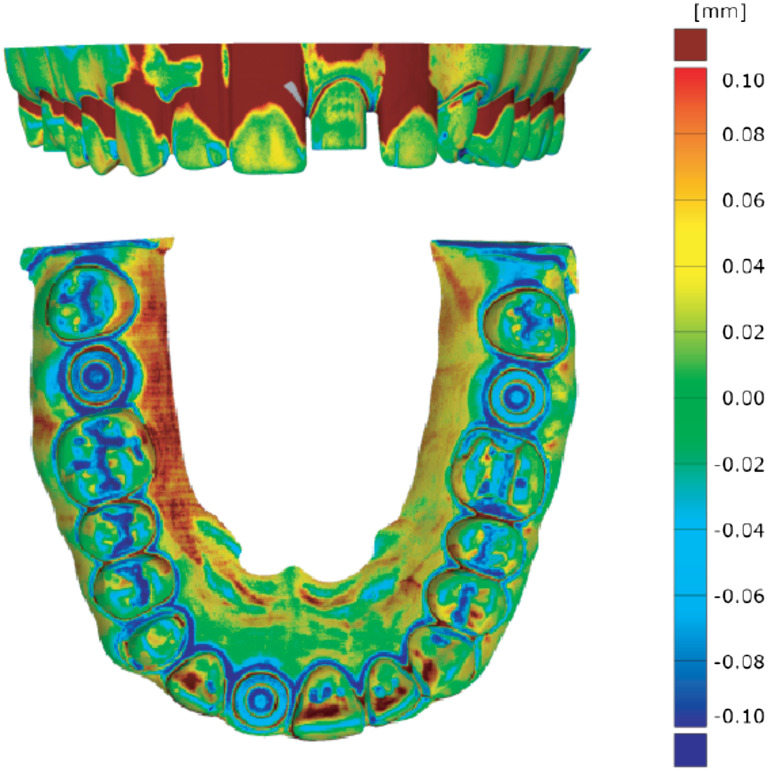
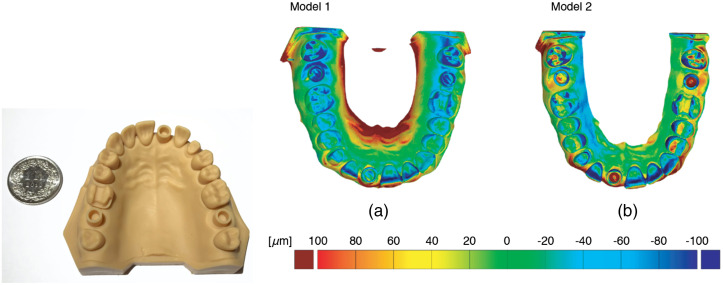
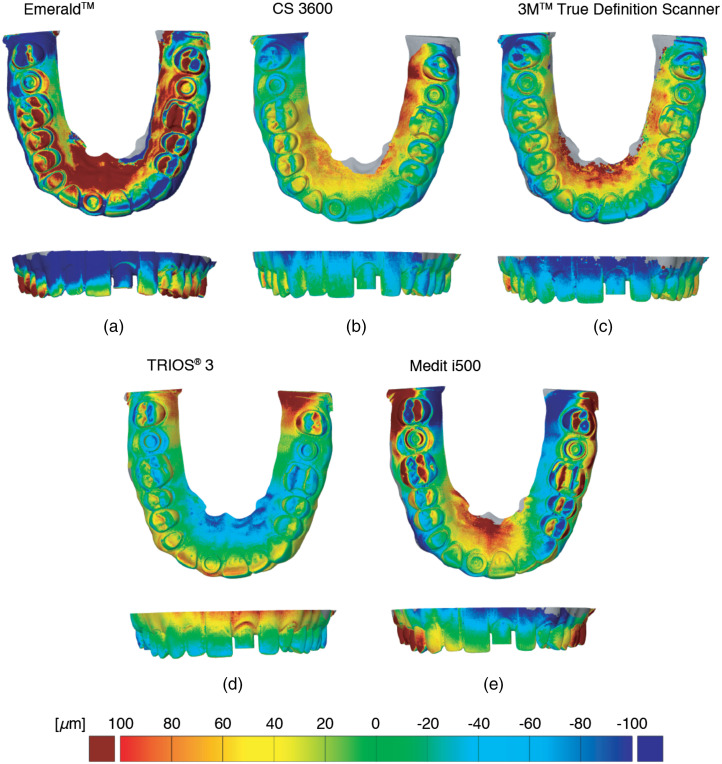
Purpose: In dental offices, there is a trend replacing conventional silicone impressions and plaster cast models by imaging data of intraoral scanners to map the denture and surrounding tissues. The aim of the study is the analysis of the accuracy of selected commercially available scanners. The accuracy is considered as the main drawback in comparison to the conventional approach. Approach: We evaluated the reproduction performance of five optical scanners by a direct comparison with high-resolution hard x-ray computed tomography data, all obtained from a polyetheretherketone model with similarity to a full-arch upper jaw. Results: Using the software GOM Inspect (GOM GmbH, Braunschweig, Germany), we could classify the intraoral scanners into two groups. The more accurate instruments gave rise to the following precision values: (TRIOS® 3, 3shape, Copenhagen, Denmark), (CS 3600, Carestream, Atlanta, Georgia), and (3M™ True Definition Scanner, 3M ESPE, St. Paul, Minnesota). The less precise systems yielded (Medit i500, Medit corp., Seongbuk-gu, South Korea) and (Emerald™, Planmeca Oy, Helsinki, Finland). Conclusions: The selected scanners are suitable for single crowns, small bridges, and separate quadrants prostheses. Scanners based on triangulation are hardly appropriate for full-arch prostheses. Besides precision, however, the choice of the scanner depends on scanning time, intraoral-camera size, and the user's learning curve. The developed protocol, which includes three-dimensional (3D) imaging and advanced computational tools for the registration with the design data, will be increasingly used in geometrical metrology by nondestructive procedures to perform dimensional measurements with micrometer precision and is capable for detailed 3D geometrical models reconstruction.
Keywords: deviation field; full-arch scanning; micro computed tomography; registration; stereolithography printer; three-dimensional accuracy evaluation.
© 2021 The Authors.
Figures
References
-
- Vögtlin C., et al. , “Comparing the accuracy of master models based on digital intra-oral scanners with conventional plaster casts,” Phys. Med. 1, 20–26 (2016).10.1016/j.phmed.2016.04.002 - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous