

Syndromic surveillance using monthly aggregate health systems information data: methods with application to COVID-19 in Liberia
- PMID: 34058004
- PMCID: PMC8195038
- DOI: 10.1093/ije/dyab094
Syndromic surveillance using monthly aggregate health systems information data: methods with application to COVID-19 in Liberia
Abstract
Background: Early detection of SARS-CoV-2 circulation is imperative to inform local public health response. However, it has been hindered by limited access to SARS-CoV-2 diagnostic tests and testing infrastructure. In regions with limited testing capacity, routinely collected health data might be leveraged to identify geographical locales experiencing higher than expected rates of COVID-19-associated symptoms for more specific testing activities.
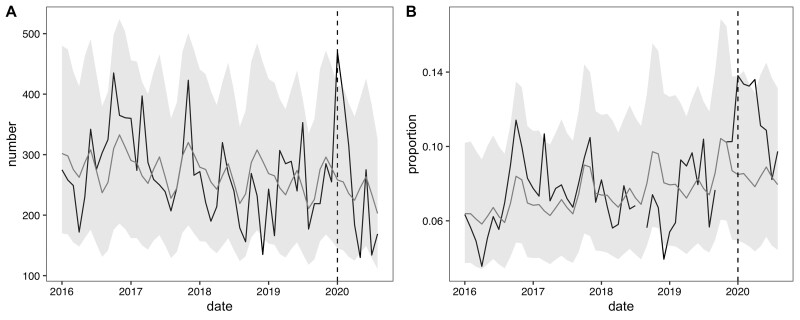
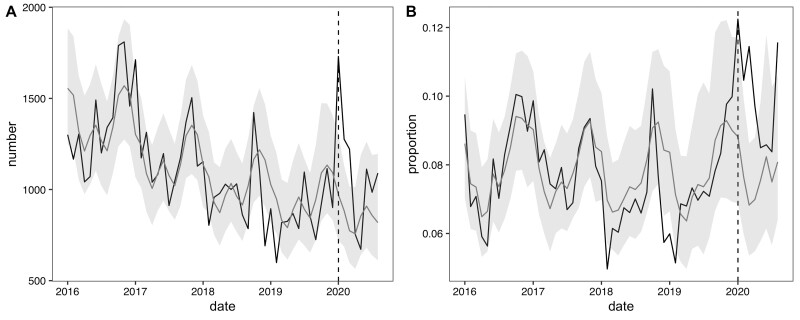
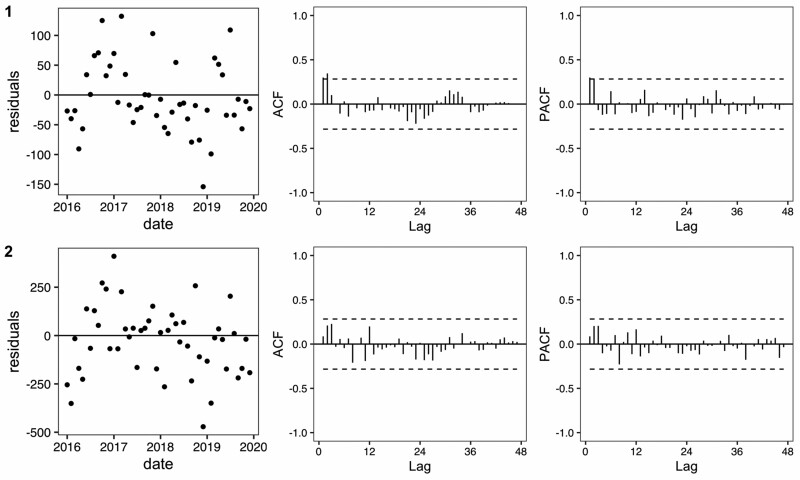
Methods: We developed syndromic surveillance tools to analyse aggregated health facility data on COVID-19-related indicators in seven low- and middle-income countries (LMICs), including Liberia. We used time series models to estimate the expected monthly counts and 95% prediction intervals based on 4 years of previous data. Here, we detail and provide resources for our data preparation procedures, modelling approach and data visualisation tools with application to Liberia.
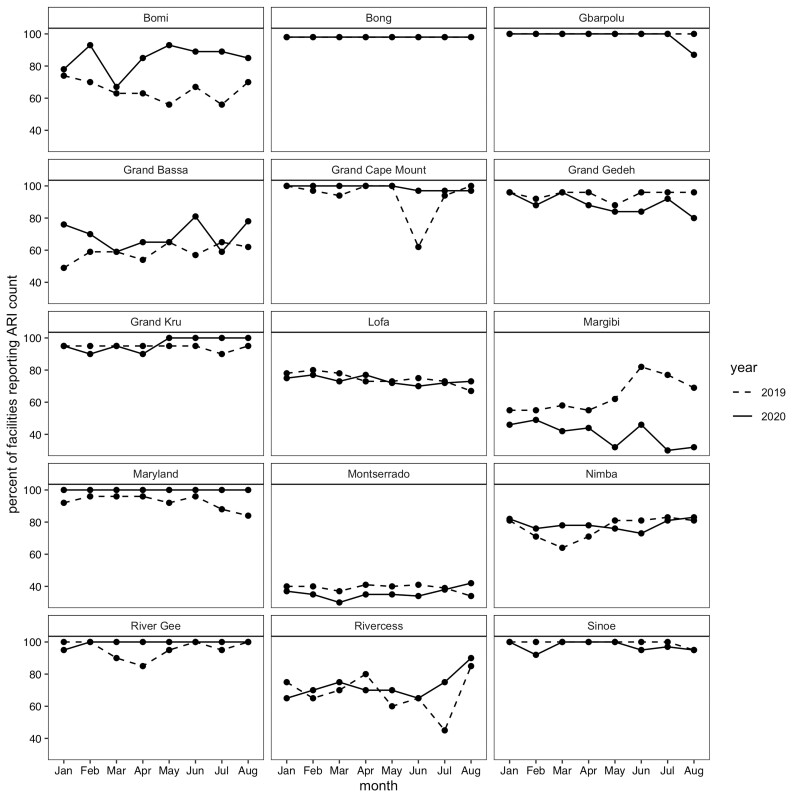
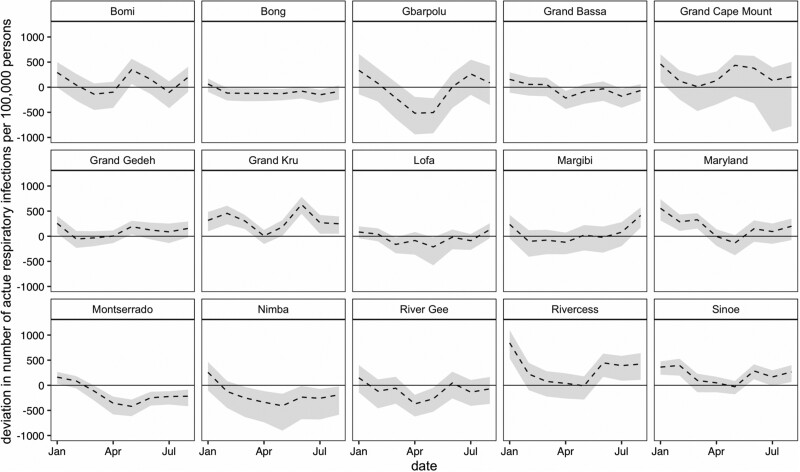
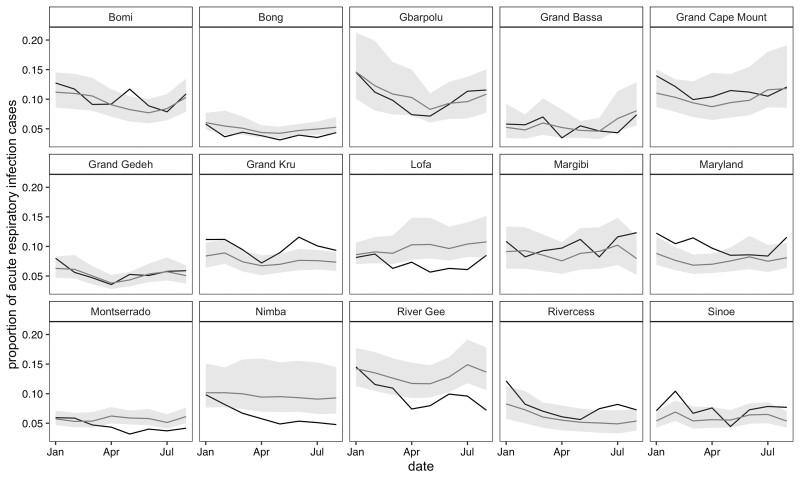
Results: To demonstrate the utility of these methods, we present syndromic surveillance results for acute respiratory infections (ARI) at health facilities in Liberia during the initial months of the COVID-19 pandemic (January through August 2020). For each month, we estimated the deviation between the expected and observed number of ARI cases for 325 health facilities and 15 counties to identify potential areas of SARS-CoV-2 circulation.
Conclusions: Syndromic surveillance can be used to monitor health facility catchment areas for spikes in specific symptoms which may indicate SARS-CoV-2 circulation. The developed methods coupled with the existing infrastructure for routine health data systems can be leveraged to monitor a variety of indicators and other infectious diseases with epidemic potential.
Keywords: COVID-19; Syndromic surveillance; disease monitoring; infectious disease; time series modelling.
© The Author(s) 2021. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures
References
-
- Davies J, Abimiku AL, Alobo M. et al. Sustainable clinical laboratory capacity for health in Africa. Lancet Glob Health 2017;5:e248–49. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
