

Natural History of Patients With Ischemia and No Obstructive Coronary Artery Disease: The CIAO-ISCHEMIA Study
- PMID: 34058845
- PMCID: PMC8478858
- DOI: 10.1161/CIRCULATIONAHA.120.046791
Natural History of Patients With Ischemia and No Obstructive Coronary Artery Disease: The CIAO-ISCHEMIA Study
Abstract
Background: Ischemia with no obstructive coronary artery disease (INOCA) is common and has an adverse prognosis. We set out to describe the natural history of symptoms and ischemia in INOCA.
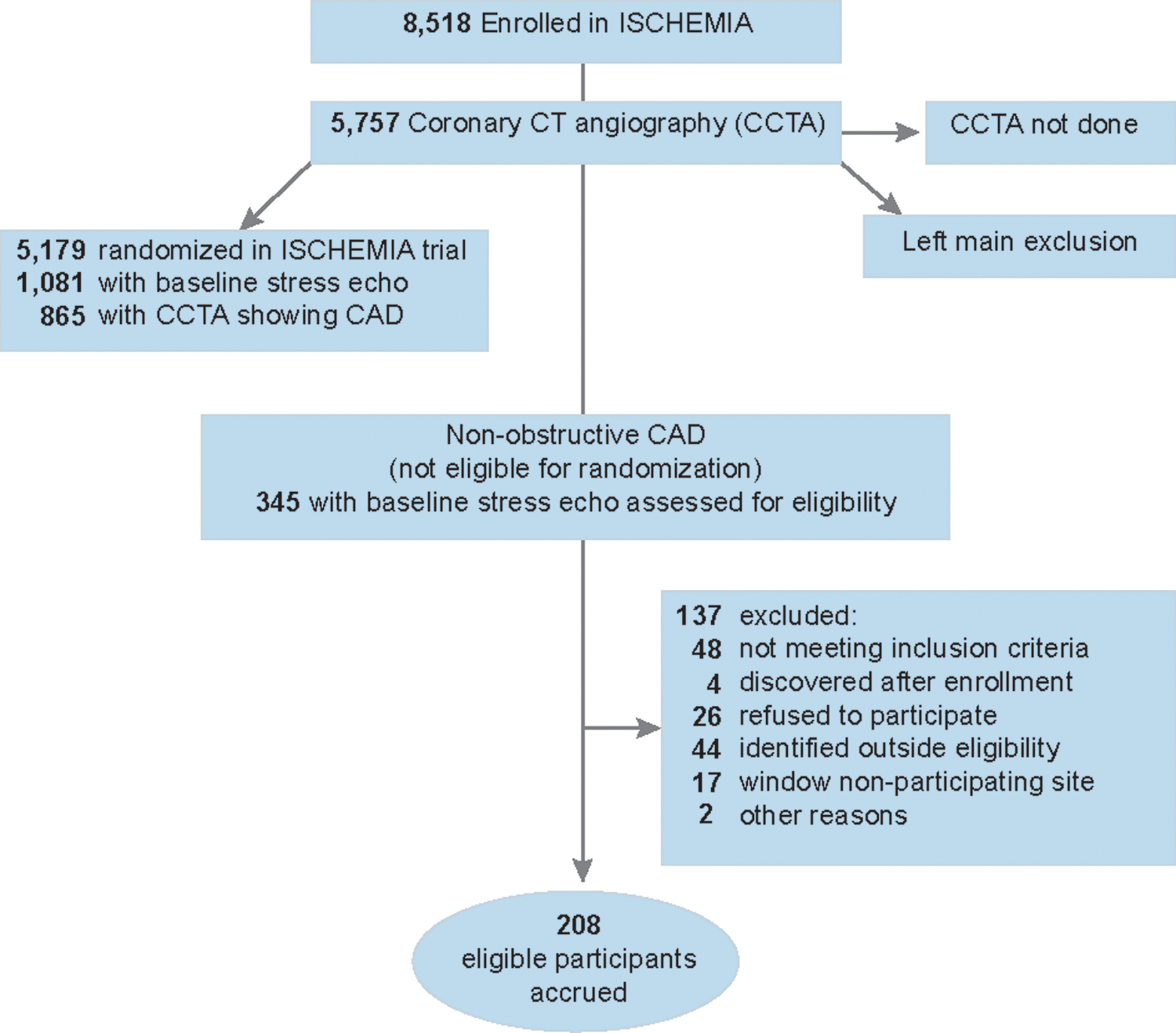
Methods: CIAO-ISCHEMIA (Changes in Ischemia and Angina over One Year in ISCHEMIA Trial Screen Failures With INOCA) was an international cohort study conducted from 2014 to 2019 involving angina assessments (Seattle Angina Questionnaire) and stress echocardiograms 1 year apart. This was an ancillary study that included patients with a history of angina who were not randomly assigned in the ISCHEMIA trial. Stress-induced wall motion abnormalities were determined by an echocardiographic core laboratory blinded to symptoms, coronary artery disease status, and test timing. Medical therapy was at the discretion of treating physicians. The primary outcome was the correlation between the changes in the Seattle Angina Questionnaire angina frequency score and changes in echocardiographic ischemia. We also analyzed predictors of 1-year changes in both angina and ischemia, and we compared CIAO participants with ISCHEMIA participants with obstructive coronary artery disease who had stress echocardiography before enrollment, as CIAO participants did.
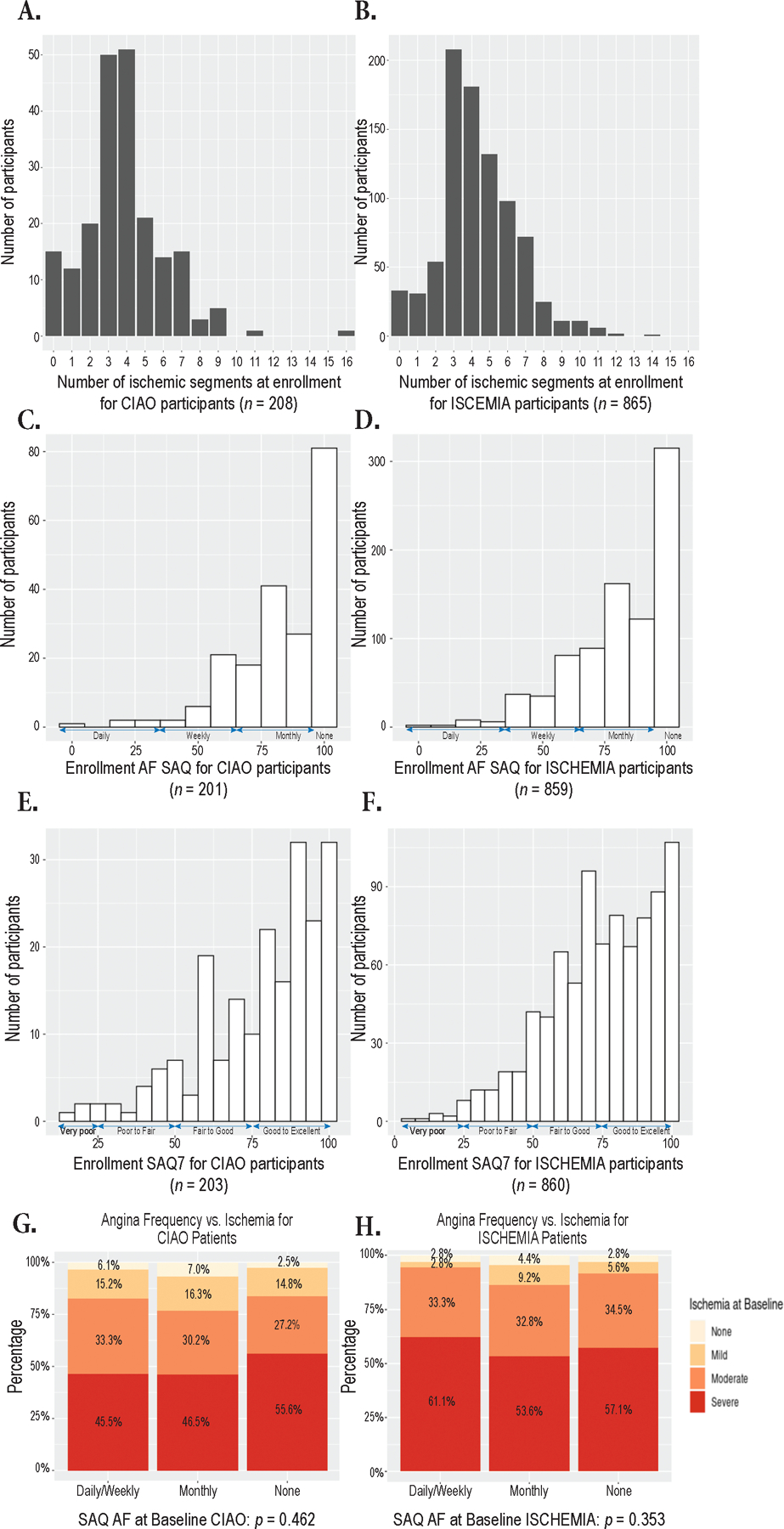
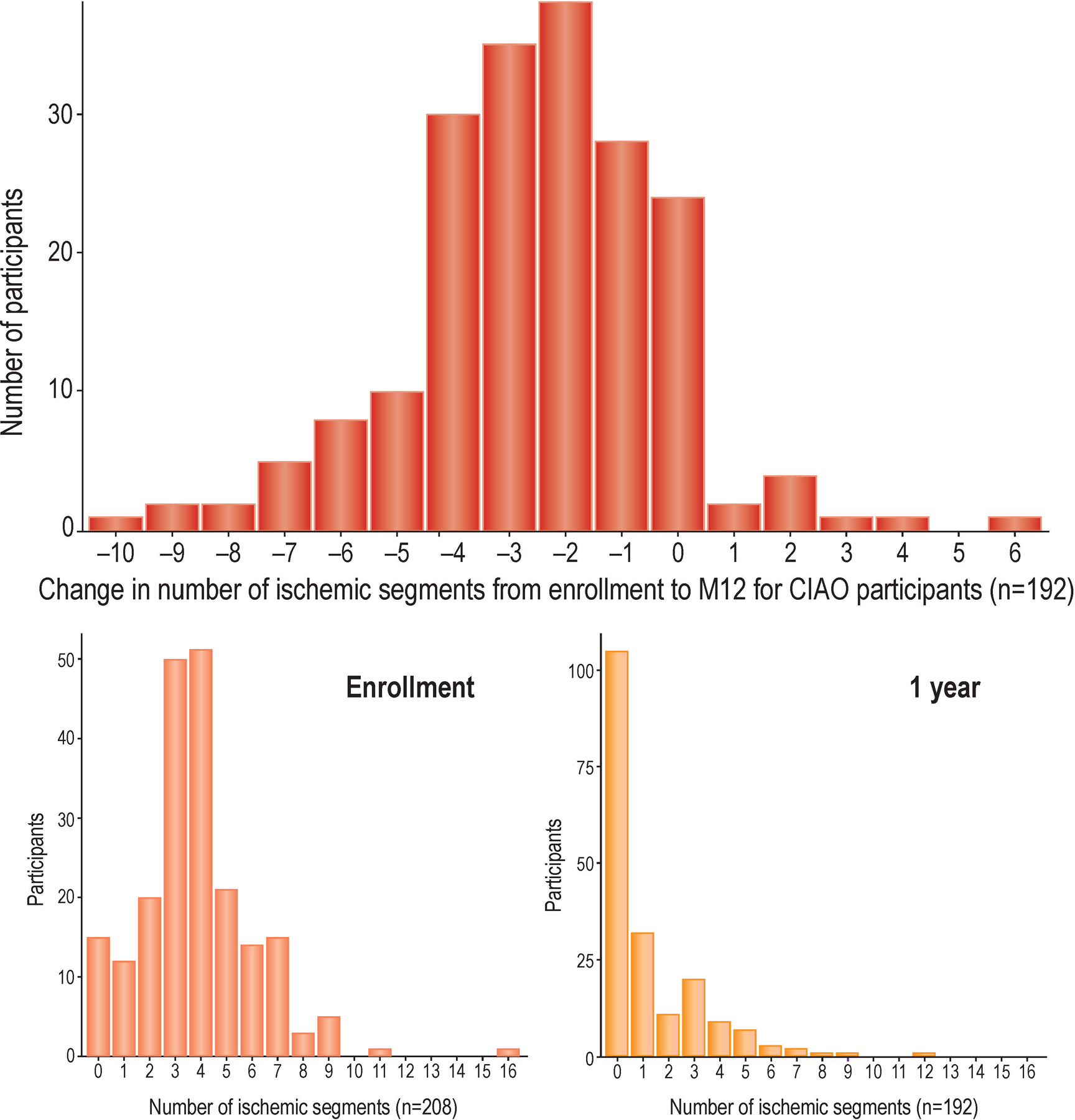
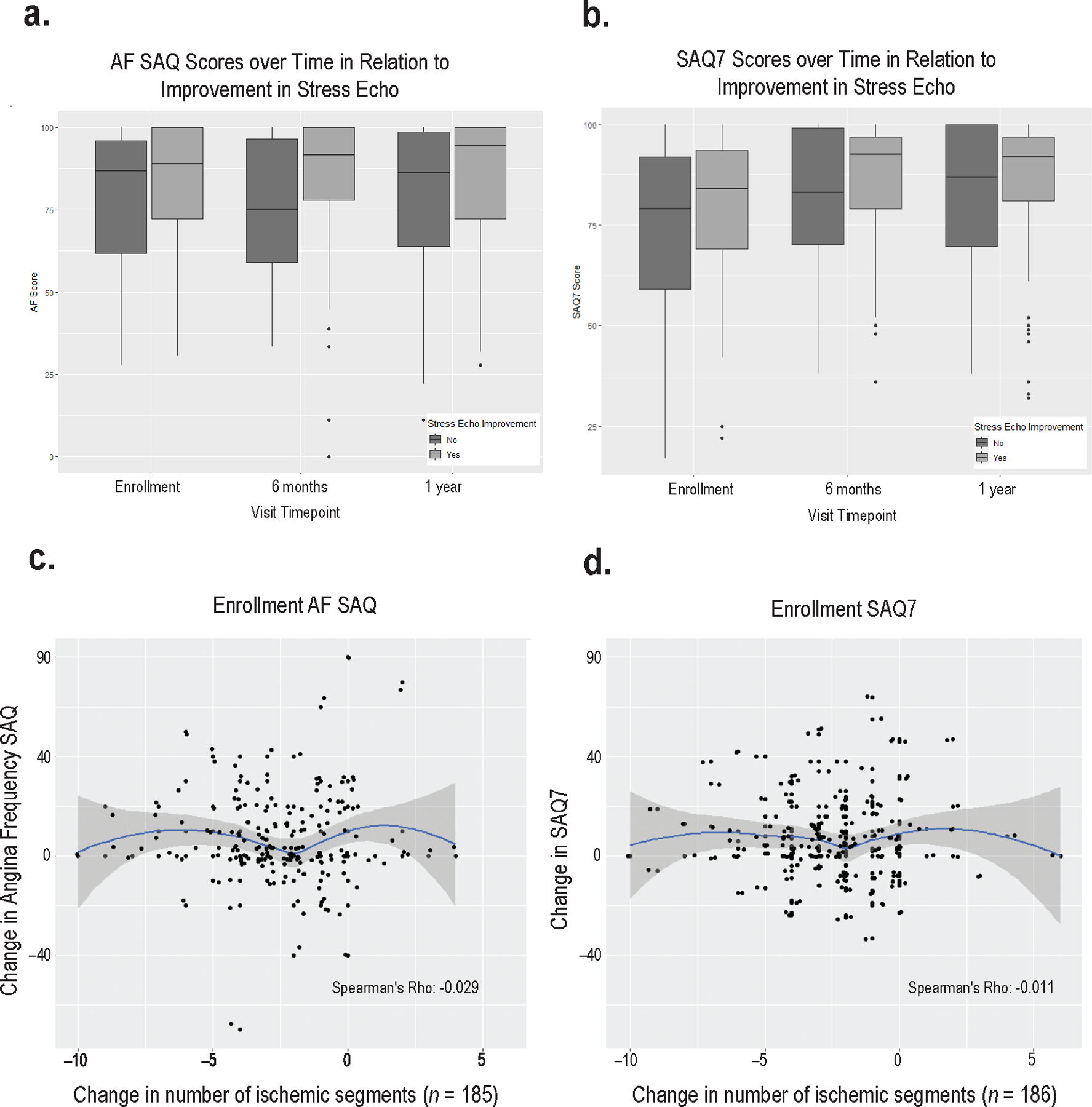
Results: INOCA participants in CIAO were more often female (66% of 208 versus 26% of 865 ISCHEMIA participants with obstructive coronary artery disease, P<0.001), but the magnitude of ischemia was similar (median 4 ischemic segments [interquartile range, 3-5] both groups). Ischemia and angina were not significantly correlated at enrollment in CIAO (P=0.46) or ISCHEMIA stress echocardiography participants (P=0.35). At 1 year, the stress echocardiogram was normal in half of CIAO participants, and 23% had moderate or severe ischemia (≥3 ischemic segments). Angina improved in 43% and worsened in 14%. Change in ischemia over 1 year was not significantly correlated with change in angina (ρ=0.029).
Conclusions: Improvement in ischemia and angina were common in INOCA but not correlated. Our INOCA cohort had a degree of inducible wall motion abnormalities similar to concurrently enrolled ISCHEMIA participants with obstructive coronary artery disease. Our results highlight the complex nature of INOCA pathophysiology and the multifactorial nature of angina. Registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT02347215.
Keywords: coronary artery disease; exercise test; ischemia; microvascular angina.
Conflict of interest statement
Conflict of Interest Disclosures
Dr. Harmony Reynolds reports grants from National Heart, Lung and Blood Institute during the conduct of the study; non-financial support from Abbott Vascular, non-financial support from BioTelemetry, outside the submitted work
Dr. Michael Picard reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. John Spertus reports grants from National Heart, Lung and Blood Institute, during the conduct of the study; personal fees from Bayer, personal fees from Novartis, personal fees from AstraZeneca, personal fees from Amgen, personal fees from Janssen, personal fees from United Healthcare, grants from American College of Cardiology, outside the submitted work; In addition, Dr. Spertus has a patent Copyright to Seattle Angina Questionnaire with royalties paid and Board of Directors for Blue Cross Blue Shield of Kansas City and Equity in Health Outcomes Sciences
Dr. Jesus Peteiro grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. Jose Luis Lopez Sendon reports grants from National Heart, Lung and Blood Institute during the conduct of the study; he also reports grants from Merck, Pfizer, and Boehringer Ingelheim outside the submitted work
Dr. Roxy Senior reports National Heart, Lung and Blood Institute during the conduct of the study; he also reports speaker fees from Lantheus Medical Imaging, Boston, Mass, Bracco, Milan, Italy, Philips Healthcare, Eindhoven, Holland
Dr. Mohammad El-Hajjar reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. Jelena Celutkiene reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. Michael Shapiro reports grants from National Heart, Lung and Blood Institute during the conduct of the study; He serves as Scientific Advisory Board for Regeneron and Amgen.
Dr. Patricia Pellikka reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. Khaled Alfakih reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. Khaled Abdul-Nour reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. Michel Khouri reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. Leonid Bershtein reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. Mark de Belder reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. Keong Kian Poh reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. John Beltrame reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Dennis Kunichoff reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Yi Li reports grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. James Min reports grants from National Heart, Lung, and Blood Institute , during the conduct of the study; other from CLEERLY INC., grants and other from GE HEALTHCARE, other from ARINETA, outside the submitted work
Dr. Jerome Fleg reports no conflict of interest
Dr. David Maron grants from National Heart, Lung and Blood Institute during the conduct of the study
Dr. Judith Hochman reports grants from National Heart, Lung, and Blood Institute during the conduct of the study; other from AstraZeneca Pharamceuticals LP, other from Arbor Pharmaceuticals LLC, other from Abbott Vascular, other from Medtronic Inc, other from St. Jude Medical Inc, other from Volcano Corp, other from Merck Sharp & Dohme Corp, other from Omron Healthcare Inc, other from Amgen Inc, during the conduct of the study
Figures
Comment in
-
Forget Ischemia: It's All About the Plaque.Circulation. 2021 Sep 28;144(13):1039-1041. doi: 10.1161/CIRCULATIONAHA.121.054102. Epub 2021 Sep 27. Circulation. 2021. PMID: 34570592 No abstract available.
References
-
- Jespersen L, Hvelplund A, Abildstrøm SZ, Pedersen F, Galatius S, Madsen JK, Jørgensen E, Kelbæk H and Prescott E. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. European Heart Journal. 2012;33:734–744. - PubMed
-
- Shaw LJ, Shaw RE, Merz CN, Brindis RG, Klein LW, Nallamothu B, Douglas PS, Krone RJ, McKay CR, Block PC, et al.Impact of ethnicity and gender differences on angiographic coronary artery disease prevalence and in-hospital mortality in the American College of Cardiology-National Cardiovascular Data Registry. Circulation. 2008;117:1787–801. - PubMed
-
- Gulati M, Cooper-DeHoff RM, McClure C, Johnson BD, Shaw LJ, Handberg EM, Zineh I, Kelsey SF, Arnsdorf MF, Black HR, et al.Adverse cardiovascular outcomes in women with nonobstructive coronary artery disease: a report from the Women’s Ischemia Syndrome Evaluation Study and the St James Women Take Heart Project. Archives of internal medicine. 2009;169:843–50. - PMC - PubMed
-
- Jespersen L, Abildstrom SZ, Hvelplund A, Madsen JK, Galatius S, Pedersen F, Hojberg S and Prescott E. Burden of hospital admission and repeat angiography in angina pectoris patients with and without coronary artery disease: a registry-based cohort study. PloS one. 2014;9:e93170–e93170. - PMC - PubMed
