

Network structure of depression and anxiety symptoms in Chinese female nursing students
- PMID: 34059013
- PMCID: PMC8168020
- DOI: 10.1186/s12888-021-03276-1
Network structure of depression and anxiety symptoms in Chinese female nursing students
Abstract
Background: Comorbidity between depressive and anxiety disorders is common. From network perspective, mental disorders arise from direct interactions between symptoms and comorbidity is due to direct interactions between depression and anxiety symptoms. The current study investigates the network structure of depression and anxiety symptoms in Chinese female nursing students and identifies the central and bridge symptoms as well as how other symptoms in present network are related to depression symptom "thoughts of death".
Methods: To understand the full spectrum of depression and anxiety, we recruited 776 Chinese female nursing students with symptoms of depression and anxiety that span the full range of normal to abnormal. Depression symptoms were measured by Patient Health Questionnaire-9 while anxiety symptoms were measured by Generalized Anxiety Disorder 7-Item Questionnaire. Network analysis was used to construct networks. Specifically, we computed the predictability, expected influence and bridge expected influence for each symptom and showed a flow network of "thoughts of death".
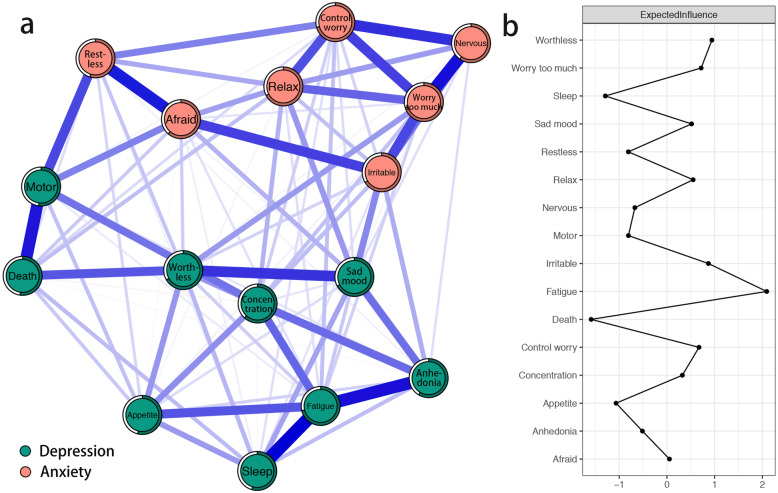
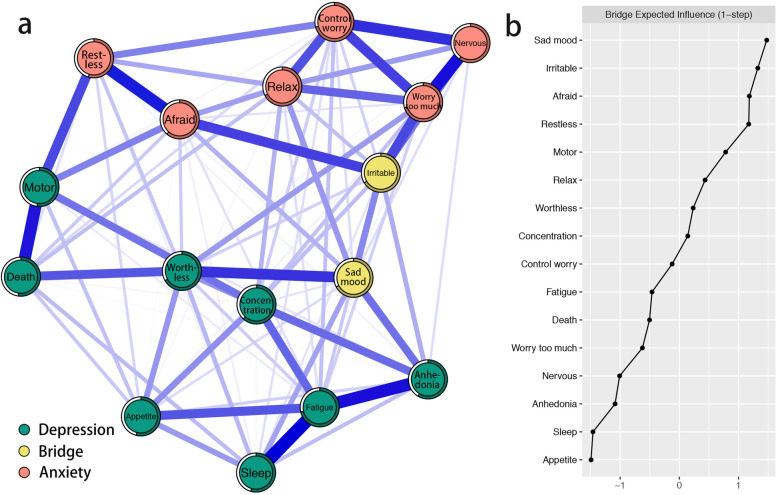
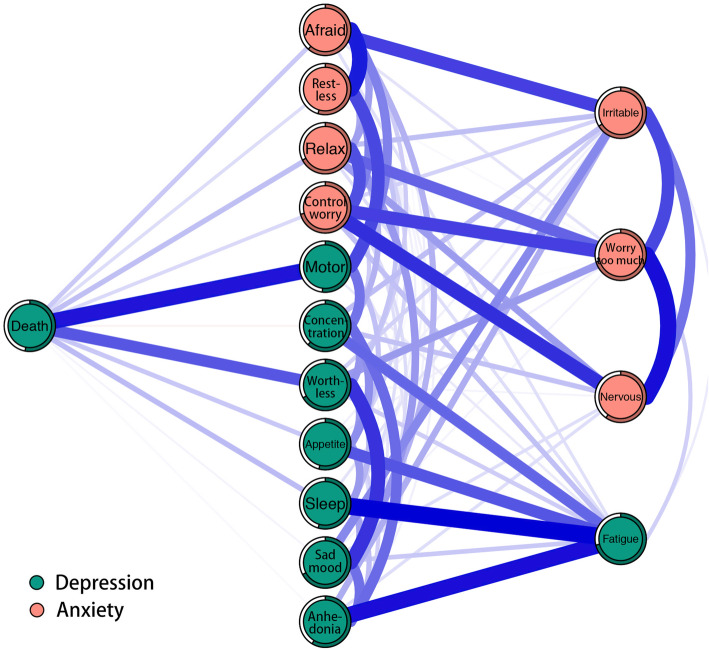
Results: Nine strongest edges existed in network were from the same disorder. Four were between depression symptoms, like "sleep difficulties" and "fatigue", and "anhedonia" and "fatigue". Five were between anxiety symptoms, like "nervousness or anxiety" and "worry too much", and "restlessness" and "afraid something will happen". The symptom "fatigue", "feeling of worthlessness" and "irritable" had the highest expected influence centrality. Results also revealed two bridge symptoms: "depressed or sad mood" and "irritable". As to "thoughts of death", the direct relations between it and "psychomotor agitation/retardation" and "feeling of worthlessness" were the strongest direct relations.
Conclusions: The current study highlighted critical central symptoms "fatigue", "feeling of worthlessness" and "irritable" and critical bridge symptoms "depressed or sad mood" and "irritable". Particularly, "psychomotor agitation/retardation" and "feeling of worthlessness" were identified as key priorities due to their strongest associations with suicide ideation. Implications for clinical prevention and intervention based on these symptoms are discussed.
Keywords: Anxiety; Comorbidity; Depression; Female nursing students; Network analysis; Suicide ideation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Network of depression and anxiety symptoms in patients with epilepsy.Epilepsy Res. 2021 Sep;175:106696. doi: 10.1016/j.eplepsyres.2021.106696. Epub 2021 Jun 23. Epilepsy Res. 2021. PMID: 34186384
-
Exploring comorbidity between anxiety and depression among migrant Filipino domestic workers: A network approach.J Affect Disord. 2019 May 1;250:85-93. doi: 10.1016/j.jad.2019.02.062. Epub 2019 Feb 26. J Affect Disord. 2019. PMID: 30836284
-
Anxiety and depression in Chinese cataract patients: a network analysis.BMC Psychol. 2024 Nov 29;12(1):709. doi: 10.1186/s40359-024-02226-2. BMC Psychol. 2024. PMID: 39614326 Free PMC article.
-
A network model of depressive and anxiety symptoms: a statistical evaluation.Mol Psychiatry. 2024 Mar;29(3):767-781. doi: 10.1038/s41380-023-02369-5. Epub 2024 Jan 18. Mol Psychiatry. 2024. PMID: 38238548 Free PMC article.
-
Prevalence of depression, anxiety and suicide among men who have sex with men in China: a systematic review and meta-analysis.Epidemiol Psychiatr Sci. 2020 Jun 15;29:e136. doi: 10.1017/S2045796020000487. Epidemiol Psychiatr Sci. 2020. PMID: 32536353 Free PMC article.
Cited by
-
The relations between different components of intolerance of uncertainty and symptoms of depression during the COVID-19 pandemic: A network analysis.Front Psychiatry. 2022 Oct 13;13:993814. doi: 10.3389/fpsyt.2022.993814. eCollection 2022. Front Psychiatry. 2022. PMID: 36311506 Free PMC article.
-
Mapping of the network connection between sleep quality symptoms, depression, generalized anxiety, and burnout in the general population of Peru and El Salvador.Psicol Reflex Crit. 2024 Jul 16;37(1):27. doi: 10.1186/s41155-024-00312-3. Psicol Reflex Crit. 2024. PMID: 39009857 Free PMC article.
-
Network connectivity between anxiety, depressive symptoms and psychological capital in Chinese university students during the COVID-19 campus closure.J Affect Disord. 2023 May 15;329:11-18. doi: 10.1016/j.jad.2023.02.087. Epub 2023 Feb 24. J Affect Disord. 2023. PMID: 36841295 Free PMC article.
-
A network analysis of difficulties in emotion regulation, anxiety, and depression for adolescents in clinical settings.Child Adolesc Psychiatry Ment Health. 2023 Feb 22;17(1):29. doi: 10.1186/s13034-023-00574-2. Child Adolesc Psychiatry Ment Health. 2023. PMID: 36814344 Free PMC article.
-
Network structure of family function and self-management in patients with early chronic kidney disease amid the COVID-19 pandemic.Front Public Health. 2023 Jan 10;10:1073409. doi: 10.3389/fpubh.2022.1073409. eCollection 2022. Front Public Health. 2023. PMID: 36703816 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
