

Intraoperative indocyanine green video angiography (ICG-VA) with FLOW 800 software in complex intracranial aneurysm surgery
- PMID: 34059164
- PMCID: PMC8168317
- DOI: 10.1186/s41016-021-00247-z
Intraoperative indocyanine green video angiography (ICG-VA) with FLOW 800 software in complex intracranial aneurysm surgery
Abstract
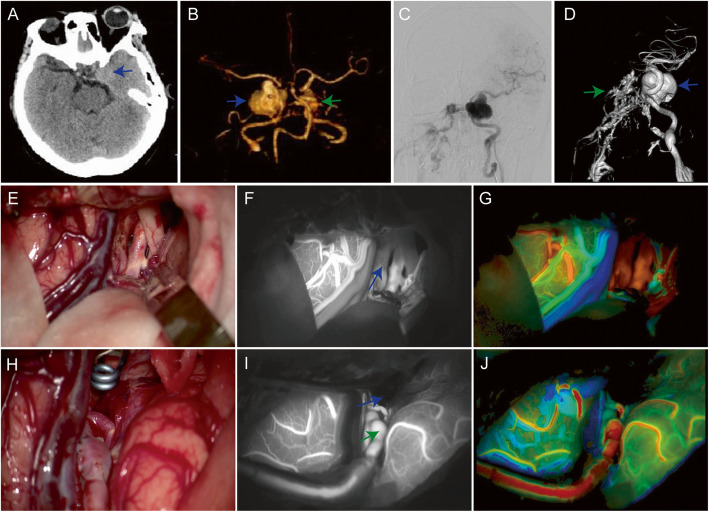
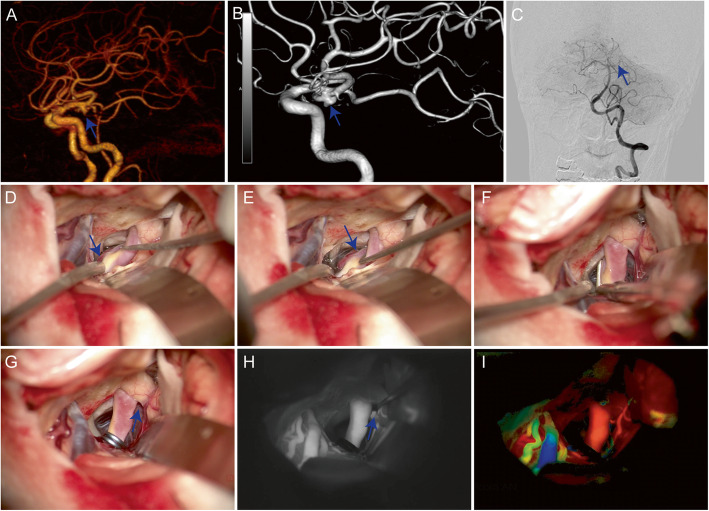
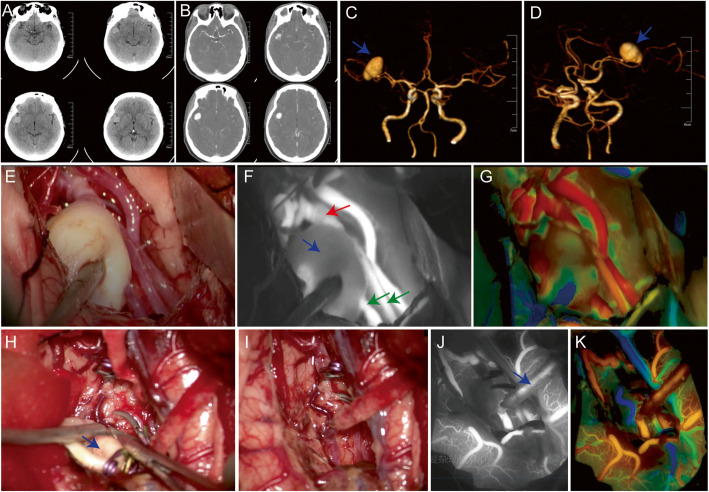
Background: Indocyanine green video angiography (ICG-VA) is a safe and effective instrument to assess changes in cerebral blood flow during cerebrovascular surgery. After ICG-VA, FLOW 800 provides a color-coded map to directly observe the dynamic distribution of blood flow and to calculate semiquantitative blood flow parameters later. The purpose of our study is to assess whether FLOW 800 is useful for surgery of complex intracranial aneurysms and to provide reliable evidence for intraoperative decision-making.
Methods: We retrospectively reviewed patients with complex aneurysms that underwent microsurgical and intraoperative evaluation of ICG-VA and FLOW 800 color-coded maps from February 2019 to May 2020. FLOW 800 data were correlated with patient characteristics, clinical outcomes, and intraoperative decision-making.
Results: The study included 32 patients with 42 complex aneurysms. All patients underwent ICG-VA FLOW 800 data provided semiquantitative data regarding localization, flow status in major feeding arteries; color maps confirmed relative adequate flow in parent, branching, and bypass vessels.
Conclusions: FLOW 800 is a useful supplement to ICG-VA for intraoperative cerebral blood flow assessment. ICG-VA and FLOW 800 can help to determine the blood flow status of the parent artery after aneurysm clipping and the bypass vessels after aneurysm bypass surgery.
Keywords: Aneurysm; Bypass; Clipping; FLOW 800; ICG-VA.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Utilizing indocyanine green video angiography to bridge intracranial aneurysm treatment gaps in low- and middle-income countries: a mini-review.J Int Med Res. 2023 Oct;51(10):3000605231204427. doi: 10.1177/03000605231204427. J Int Med Res. 2023. PMID: 37862677 Free PMC article. Review.
-
Application of Intraoperative FLOW 800 Indocyanine Green Videoangiography Color-Coded Maps for Microsurgical Clipping of Intracranial Aneurysms.World Neurosurg. 2019 Nov;131:e192-e200. doi: 10.1016/j.wneu.2019.07.113. Epub 2019 Jul 19. World Neurosurg. 2019. PMID: 31330337
-
Complementary role of Indocyanine green video angiography, dual-image video angiography and flow-800.Br J Neurosurg. 2023 Dec;37(6):1652-1658. doi: 10.1080/02688697.2023.2207648. Epub 2023 May 3. Br J Neurosurg. 2023. PMID: 37132265
-
The Application of FLOW 800 ICG Videoangiography Color Maps for Neurovascular Surgery and Intraoperative Decision Making.World Neurosurg. 2019 Feb;122:e186-e197. doi: 10.1016/j.wneu.2018.09.195. Epub 2018 Oct 5. World Neurosurg. 2019. PMID: 30292668
-
Essentials in intraoperative indocyanine green videoangiography assessment for intracranial aneurysm surgery: conclusions from 295 consecutively clipped aneurysms and review of the literature.Neurosurg Focus. 2014 Feb;36(2):E7. doi: 10.3171/2013.11.FOCUS13475. Neurosurg Focus. 2014. PMID: 24484260 Review.
Cited by
-
Utilizing indocyanine green video angiography to bridge intracranial aneurysm treatment gaps in low- and middle-income countries: a mini-review.J Int Med Res. 2023 Oct;51(10):3000605231204427. doi: 10.1177/03000605231204427. J Int Med Res. 2023. PMID: 37862677 Free PMC article. Review.
-
Dual Microscope Indocyanine Green Video Angiography and Endoscopic Review to Treat Intracranial Aneurysm: A Review of the Literature Regarding a Case.Asian J Neurosurg. 2023 Nov 30;18(4):701-707. doi: 10.1055/s-0043-1775584. eCollection 2023 Dec. Asian J Neurosurg. 2023. PMID: 38161615 Free PMC article. Review.
-
Clinical characteristics and treatment strategies for pituitary adenoma associated with intracranial aneurysm.Chin Neurosurg J. 2024 Jun 4;10(1):18. doi: 10.1186/s41016-024-00370-7. Chin Neurosurg J. 2024. PMID: 38835088 Free PMC article.
-
Complex intracranial aneurysms: a DELPHI study to define associated characteristics.Acta Neurochir (Wien). 2024 Jul 11;166(1):294. doi: 10.1007/s00701-024-06182-z. Acta Neurochir (Wien). 2024. PMID: 38990336
-
ICG Flow 800 technology targeted STA-MCA microvascular bypass for exclusion of deep-seated fusiform MCA aneurysm: 2-dimensional operative video.Neurosurg Focus Video. 2022 Jan 1;6(1):V14. doi: 10.3171/2021.10.FOCVID21183. eCollection 2022 Jan. Neurosurg Focus Video. 2022. PMID: 36284596 Free PMC article.
References
-
- Hanel RA, Spetzler RF. Surgical treatment of complex intracranial aneurysms [J] Neurosurgery. 2008;62(6 Suppl 3):1289–1297. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources