

New risk model is able to identify patients with a low risk of progression in systemic sclerosis
- PMID: 34059523
- PMCID: PMC8169494
- DOI: 10.1136/rmdopen-2020-001524
New risk model is able to identify patients with a low risk of progression in systemic sclerosis
Abstract
Objectives: To develop a prediction model to guide annual assessment of systemic sclerosis (SSc) patients tailored in accordance to disease activity.
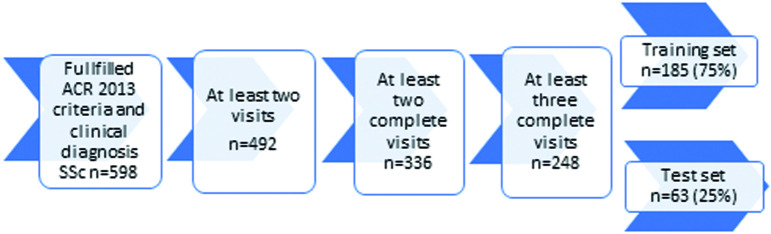
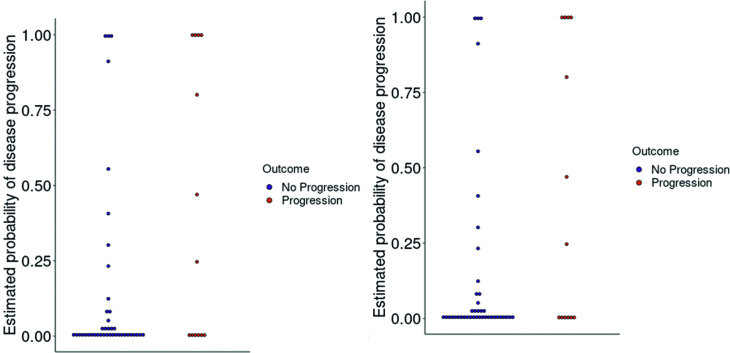
Methods: A machine learning approach was used to develop a model that can identify patients without disease progression. SSc patients included in the prospective Leiden SSc cohort and fulfilling the ACR/EULAR 2013 criteria were included. Disease progression was defined as progression in ≥1 organ system, and/or start of immunosuppression or death. Using elastic-net-regularisation, and including 90 independent clinical variables (100% complete), we trained the model on 75% and validated it on 25% of the patients, optimising on negative predictive value (NPV) to minimise the likelihood of missing progression. Probability cutoffs were identified for low and high risk for disease progression by expert assessment.
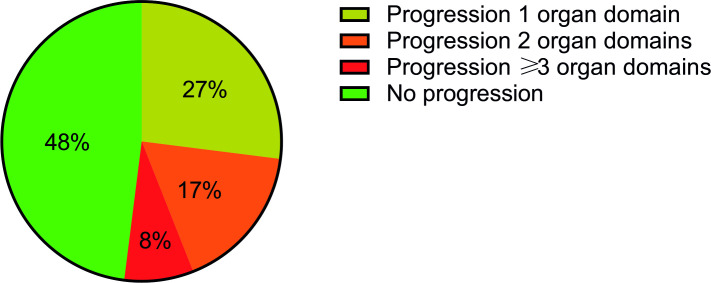
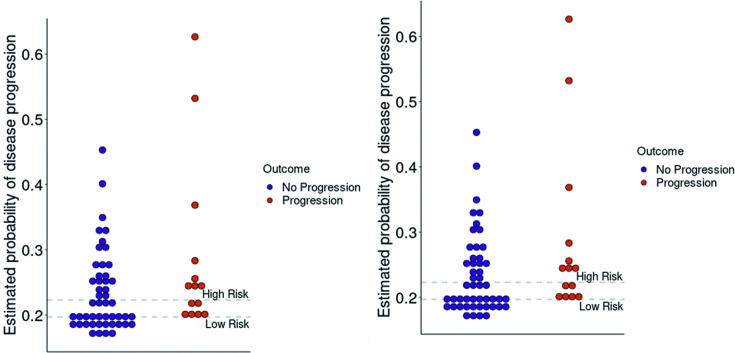
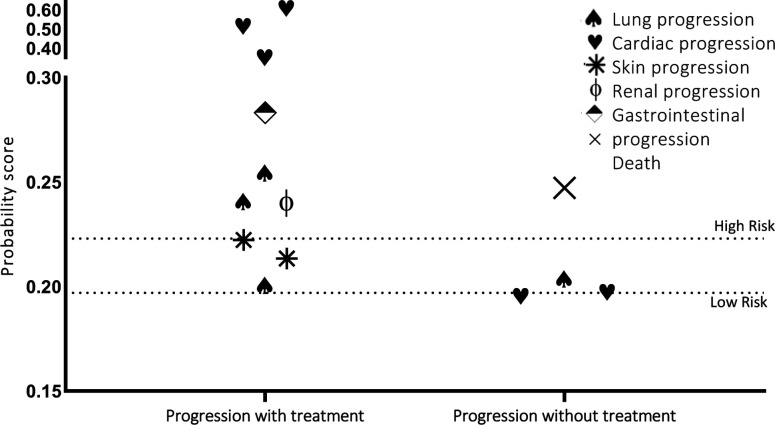
Results: Of the 492 SSc patients (follow-up range: 2-10 years), disease progression during follow-up was observed in 52% (median time 4.9 years). Performance of the model in the test set showed an AUC-ROC of 0.66. Probability score cutoffs were defined: low risk for disease progression (<0.197, NPV:1.0; 29% of patients), intermediate risk (0.197-0.223, NPV:0.82; 27%) and high risk (>0.223, NPV:0.78; 44%). The relevant variables for the model were: previous use of cyclophosphamide or corticosteroids, start with immunosuppressive drugs, previous gastrointestinal progression, previous cardiovascular event, pulmonary arterial hypertension, modified Rodnan Skin Score, creatine kinase and diffusing capacity for carbon monoxide.
Conclusion: Our machine-learning-assisted model for progression enabled us to classify 29% of SSc patients as 'low risk'. In this group, annual assessment programmes could be less extensive than indicated by international guidelines.
Keywords: autoimmunity; health care; outcome assessment; scleroderma; systemic.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Systemic sclerosis associated interstitial lung disease - individualized immunosuppressive therapy and course of lung function: results of the EUSTAR group.Arthritis Res Ther. 2018 Jan 30;20(1):17. doi: 10.1186/s13075-018-1517-z. Arthritis Res Ther. 2018. PMID: 29382380 Free PMC article.
-
Associations with digital ulcers in a large cohort of systemic sclerosis: results from the Canadian Scleroderma Research Group registry.Arthritis Care Res (Hoboken). 2011 Jan;63(1):142-9. doi: 10.1002/acr.20336. Arthritis Care Res (Hoboken). 2011. PMID: 20740608
-
Validation of the 2013 American College of Rheumatology/European League Against Rheumatism classification criteria for systemic sclerosis in patients from a capillaroscopy clinic.Semin Arthritis Rheum. 2016 Dec;46(3):350-355. doi: 10.1016/j.semarthrit.2016.05.007. Epub 2016 Jun 3. Semin Arthritis Rheum. 2016. PMID: 27373498
-
Scleroderma in children.Best Pract Res Clin Rheumatol. 2017 Aug;31(4):576-595. doi: 10.1016/j.berh.2018.02.004. Epub 2018 Mar 27. Best Pract Res Clin Rheumatol. 2017. PMID: 29773274 Review.
-
Safety and efficacy of Rituximab in systemic sclerosis: A systematic review and meta-analysis.Int Immunopharmacol. 2020 Jun;83:106389. doi: 10.1016/j.intimp.2020.106389. Epub 2020 Mar 12. Int Immunopharmacol. 2020. PMID: 32172205
Cited by
-
Over-the-Counter Breast Cancer Classification Using Machine Learning and Patient Registration Records.Diagnostics (Basel). 2022 Nov 16;12(11):2826. doi: 10.3390/diagnostics12112826. Diagnostics (Basel). 2022. PMID: 36428886 Free PMC article.
-
Latent trajectory modelling of pulmonary artery pressure in systemic sclerosis: a retrospective cohort study.RMD Open. 2022 Dec;8(2):e002673. doi: 10.1136/rmdopen-2022-002673. RMD Open. 2022. PMID: 36581382 Free PMC article.
-
The Use and Utility of Machine Learning in Achieving Precision Medicine in Systemic Sclerosis: A Narrative Review.J Pers Med. 2022 Jul 23;12(8):1198. doi: 10.3390/jpm12081198. J Pers Med. 2022. PMID: 35893293 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical