

Imaging findings of trichilemmal cyst and proliferating trichilemmal tumour
- PMID: 34060944
- PMCID: PMC8649188
- DOI: 10.1177/19714009211017789
Imaging findings of trichilemmal cyst and proliferating trichilemmal tumour
Abstract
Purpose: The purpose of this study was to evaluate computed tomography and magnetic resonance imaging of benign trichilemmal cysts and proliferating trichilemmal tumours.
Methods: Nineteen histologically confirmed cutaneous lesions with trichilemmal keratinisation (12 trichilemmal cysts and seven proliferating trichilemmal tumours) were enrolled. Among them, 10 lesions (six trichilemmal cysts and four proliferating trichilemmal tumours) were examined by computed tomography, while 13 lesions (eight trichilemmal cysts and five proliferating trichilemmal tumours) were examined by magnetic resonance imaging. Computed tomography and magnetic resonance imaging characteristics were retrospectively reviewed.
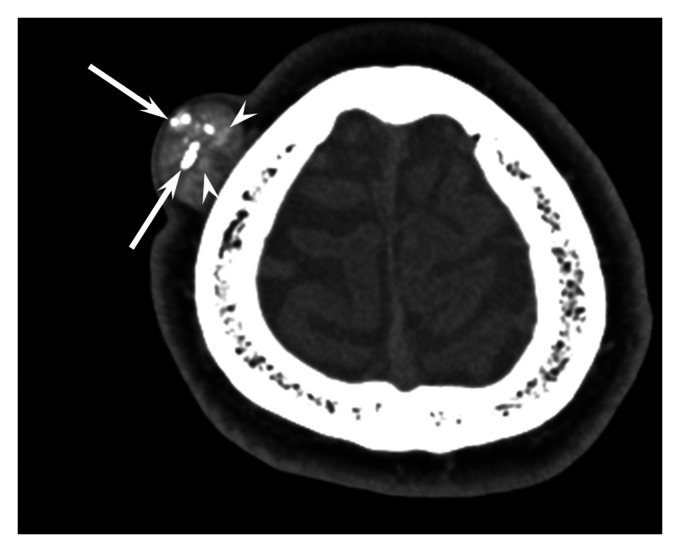
Results: Sixteen lesions (84%, 10 trichilemmal cysts and six proliferating trichilemmal tumours) occurred on the scalp. Lobulated margins were observed in five lesions (26%, three trichilemmal cysts and two proliferating trichilemmal tumours). With respect to computed tomography attenuation, calcification (>200 Hounsfield units) was observed in seven lesions (70%, five trichilemmal cysts and two proliferating trichilemmal tumours), hyperdense areas (≥80 and ≤200 Hounsfield units) in six (60%, three trichilemmal cysts and three proliferating trichilemmal tumours), and soft tissue density areas (<80 Hounsfield units) in nine (90%, five trichilemmal cysts and four proliferating trichilemmal tumours). On T1-weighted images, intratumoral hyperintensity was only observed in eight trichilemmal cysts but no proliferating trichilemmal tumours (100% vs. 0%, P<0.01). On T2-weighted images, hypointense rim and intratumoral hypointensity was observed in all 13 lesions (100%, eight trichilemmal cysts and five proliferating trichilemmal tumours), and linear or reticular hypointensity was observed in 10 (77%, six trichilemmal cysts and four proliferating trichilemmal tumours).
Conclusion: Trichilemmal cysts and proliferating trichilemmal tumours predominantly occurred on the scalp with calcification, and usually exhibited linear or reticular T2 hypointensity. Intratumoral T1 hyperintensity may be a useful imaging feature for differentiating trichilemmal cysts from proliferating trichilemmal tumours.
Keywords: CT; MRI; Trichilemmal cyst; proliferating trichilemmal tumour; scalp.
Conflict of interest statement
Figures



Similar articles
-
Trichilemmal Cyst: Clinical and Sonographic Features.J Ultrasound Med. 2019 Jan;38(1):91-96. doi: 10.1002/jum.14666. Epub 2018 Apr 30. J Ultrasound Med. 2019. PMID: 29708283
-
Proliferating trichilemmal cyst.J Cutan Pathol. 1983 Jun;10(3):178-87. doi: 10.1111/j.1600-0560.1983.tb00324.x. J Cutan Pathol. 1983. PMID: 6863684
-
Malignant Proliferating Trichilemmal Tumour of the Scalp with Intra-Cranial Extension and Lung Metastasis-a Case Report.Indian J Surg. 2016 Dec;78(6):493-495. doi: 10.1007/s12262-015-1427-0. Epub 2016 Jan 15. Indian J Surg. 2016. PMID: 28100948 Free PMC article.
-
Proliferating trichilemmal tumors: a review of the literature.Dermatol Surg. 2007 Sep;33(9):1102-8. doi: 10.1111/j.1524-4725.2007.33225.x. Dermatol Surg. 2007. PMID: 17760602 Review.
-
Two Cases of Malignant Proliferating Trichilemmal Tumor (MPTT) and Review of Literature.R I Med J (2013). 2022 Feb 1;105(1):12-16. R I Med J (2013). 2022. PMID: 35081182 Review.
Cited by
-
The Incidental Finding of Trichilemmal Cyst in a Patient With Acute Kidney Injury.Cureus. 2024 Jul 16;16(7):e64657. doi: 10.7759/cureus.64657. eCollection 2024 Jul. Cureus. 2024. PMID: 39149657 Free PMC article.
-
Rare Case of Giant Proliferating Trichilemmal Tumor Behind Left Shoulder: A Case Report.Clin Case Rep. 2025 Jan 2;13(1):e70040. doi: 10.1002/ccr3.70040. eCollection 2025 Jan. Clin Case Rep. 2025. PMID: 39759184 Free PMC article.
-
Malignant proliferative ependymoma of the neck with lymph node metastasis: A case report.World J Clin Cases. 2023 Oct 6;11(28):6949-6954. doi: 10.12998/wjcc.v11.i28.6949. World J Clin Cases. 2023. PMID: 37901030 Free PMC article.
-
A Case of a Giant Trichilemmal Cyst on the Forehead.J Plast Reconstr Surg. 2023 Jul 31;3(1):21-25. doi: 10.53045/jprs.2022-0044. eCollection 2024 Jan 27. J Plast Reconstr Surg. 2023. PMID: 40104413 Free PMC article.
-
An unusual pathology of a nasal tip mass in a 28-year-old female.Radiol Case Rep. 2025 Jan 23;20(4):1972-1974. doi: 10.1016/j.radcr.2024.12.061. eCollection 2025 Apr. Radiol Case Rep. 2025. PMID: 39926267 Free PMC article.
References
-
- Requena L, Crowson AN, Kaddu S, et al.. Proliferating trichilemmal tumor. In: WHO Classification of Skin Tumors 4. Lyon, France: IARC Press, 2018, pp. 196–197.
-
- Kawaguchi M, Kato H, Matsuo M. CT and MRI features of scalp lesions. Radiol Med 2019; 124: 1049–1061. DOI: 10.1007/s11547-019-01060-6 - PubMed
-
- Prodinger CM, Koller J, Laimer M. Scalp tumors. J Dtsch Dermatol Ges 2018; 16: 730–753. 2018/06/07. DOI: 10.1111/ddg.13546 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
