

Effect of Reduced-Dose vs High-Dose Glucocorticoids Added to Rituximab on Remission Induction in ANCA-Associated Vasculitis: A Randomized Clinical Trial
- PMID: 34061144
- PMCID: PMC8170547
- DOI: 10.1001/jama.2021.6615
Effect of Reduced-Dose vs High-Dose Glucocorticoids Added to Rituximab on Remission Induction in ANCA-Associated Vasculitis: A Randomized Clinical Trial
Abstract
Importance: The current standard induction therapy for antineutrophil cytoplasm antibody (ANCA)-associated vasculitis is the combination of high-dose glucocorticoids and cyclophosphamide or rituximab. Although these regimens have high remission rates, they are associated with considerable adverse events presumably due to high-dose glucocorticoids.
Objective: To compare efficacy and adverse events between a reduced-dose glucocorticoid plus rituximab regimen and the standard high-dose glucocorticoid plus rituximab regimen in remission induction of ANCA-associated vasculitis.
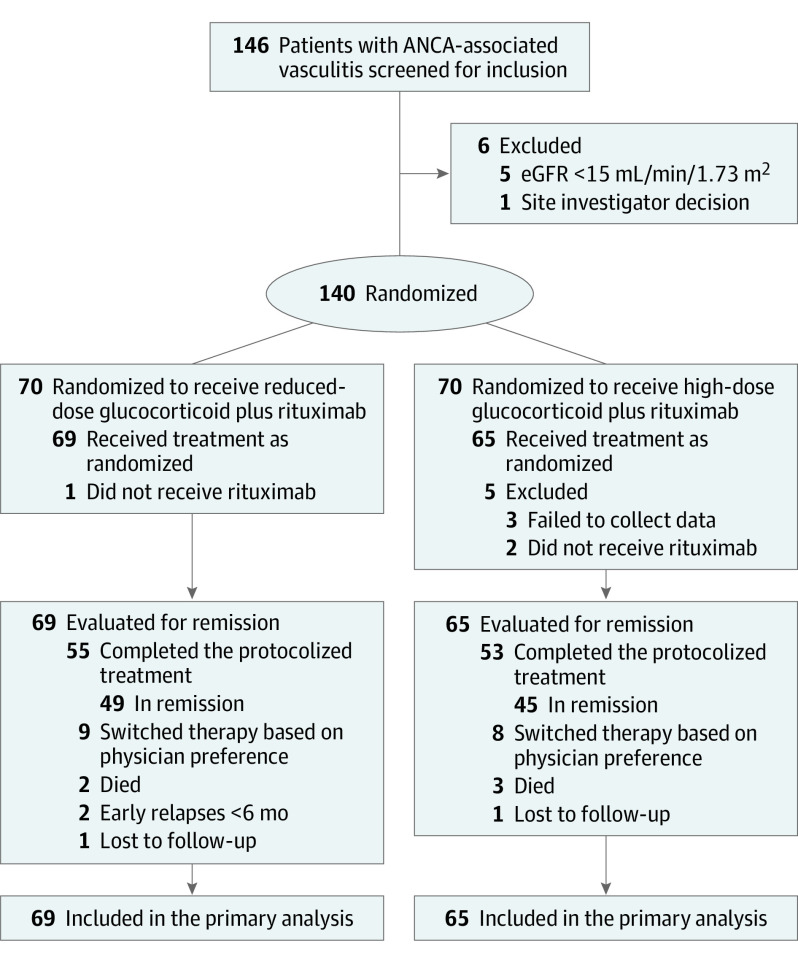
Design, setting, and participants: This was a phase 4, multicenter, open-label, randomized, noninferiority trial. A total of 140 patients with newly diagnosed ANCA-associated vasculitis without severe glomerulonephritis or alveolar hemorrhage were enrolled between November 2014 and June 2019 at 21 hospitals in Japan. Follow-up ended in December 2019.
Interventions: Patients were randomized to receive reduced-dose prednisolone (0.5 mg/kg/d) plus rituximab (375 mg/m2/wk, 4 doses) (n = 70) or high-dose prednisolone (1 mg/kg/d) plus rituximab (n = 70).
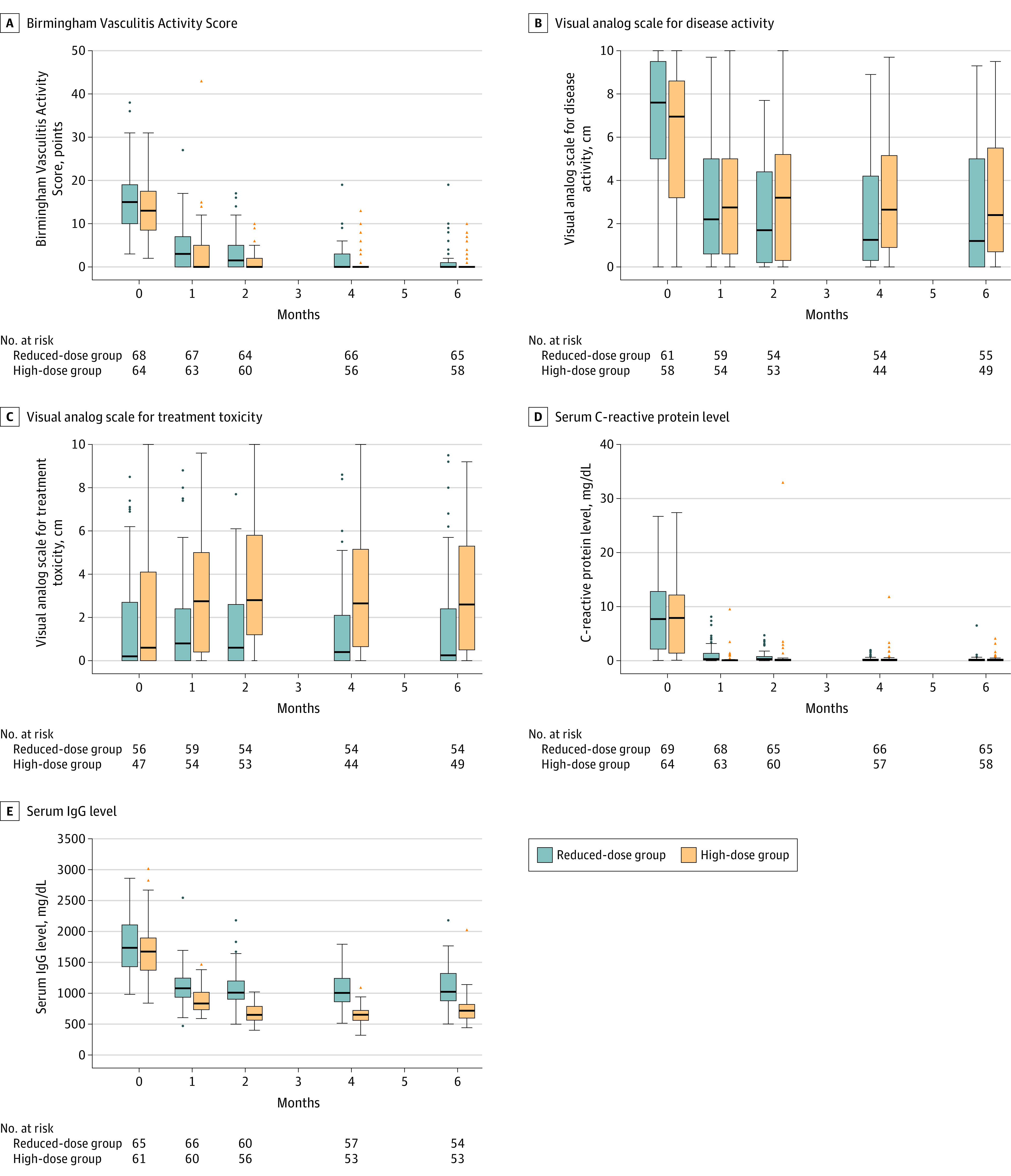
Main outcomes and measures: The primary end point was the remission rate at 6 months, and the prespecified noninferiority margin was -20 percentage points. There were 8 secondary efficacy outcomes and 6 secondary safety outcomes, including serious adverse events and infections.
Results: Among 140 patients who were randomized (median age, 73 years; 81 women [57.8%]), 134 (95.7%) completed the trial. At 6 months, 49 of 69 patients (71.0%) in the reduced-dose group and 45 of 65 patients (69.2%) in the high-dose group achieved remission with the protocolized treatments. The treatment difference of 1.8 percentage points (1-sided 97.5% CI, -13.7 to ∞) between the groups met the noninferiority criterion (P = .003 for noninferiority). Twenty-one serious adverse events occurred in 13 patients in the reduced-dose group (18.8%), while 41 occurred in 24 patients in the high-dose group (36.9%) (difference, -18.1% [95% CI, -33.0% to -3.2%]; P = .02). Seven serious infections occurred in 5 patients in the reduced-dose group (7.2%), while 20 occurred in 13 patients in the high-dose group (20.0%) (difference, -12.8% [95% CI, -24.2% to -1.3%]; P = .04).
Conclusions and relevance: Among patients with newly diagnosed ANCA-associated vasculitis without severe glomerulonephritis or alveolar hemorrhage, a reduced-dose glucocorticoid plus rituximab regimen was noninferior to a high-dose glucocorticoid plus rituximab regimen with regard to induction of disease remission at 6 months.
Trial registration: ClinicalTrials.gov Identifier: NCT02198248.
Conflict of interest statement
Figures
Comment in
-
Reduced-Dose vs High-Dose Glucocorticoids Added to Rituximab and Remission Induction in ANCA-Associated Vasculitis.JAMA. 2021 Oct 19;326(15):1536. doi: 10.1001/jama.2021.13873. JAMA. 2021. PMID: 34665208 No abstract available.
-
Reduced-Dose vs High-Dose Glucocorticoids Added to Rituximab and Remission Induction in ANCA-Associated Vasculitis.JAMA. 2021 Oct 19;326(15):1535-1536. doi: 10.1001/jama.2021.13867. JAMA. 2021. PMID: 34665209 No abstract available.
-
Reduced-Dose vs High-Dose Glucocorticoids Added to Rituximab and Remission Induction in ANCA-Associated Vasculitis.JAMA. 2021 Oct 19;326(15):1535. doi: 10.1001/jama.2021.13863. JAMA. 2021. PMID: 34665210 No abstract available.
References
-
- Harigai M, Nagasaka K, Amano K, et al. 2017 Clinical practice guidelines of the Japan Research Committee of the Ministry of Health, Labour, and Welfare for Intractable Vasculitis for the management of ANCA-associated vasculitis. Mod Rheumatol. 2019;29(1):20-30. doi: 10.1080/14397595.2018.1500437 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
