

What Are the Long-term Outcomes of Mortality, Quality of Life, and Hip Function after Prosthetic Joint Infection of the Hip? A 10-year Follow-up from Sweden
- PMID: 34061486
- PMCID: PMC8445574
- DOI: 10.1097/CORR.0000000000001838
What Are the Long-term Outcomes of Mortality, Quality of Life, and Hip Function after Prosthetic Joint Infection of the Hip? A 10-year Follow-up from Sweden
Abstract
Background: Prosthetic joint infection (PJI) is a complication after arthroplasty that negatively affects patient health. However, prior reports have not addressed the long-term consequences of hip PJI in terms of patient mortality, quality of life, and hip function.
Questions/purposes: At a minimum of 10 years after PJI in patients undergoing primary THA, in the context of several large, national databases in Sweden, we asked: (1) Is mortality increased for patients with PJI after THA compared with patients with a noninfected THA? (2) Does PJI of the hip have a negative influence on quality of life as measured by the Euro-QoL-5D-5L (EQ-5D-5L), ambulatory aids, residential status, and hip function as measured by the Oxford Hip Score (OHS)? (3) Which factors are associated with poor patient-reported outcome measures (PROMs) for patients with PJI after primary THA?
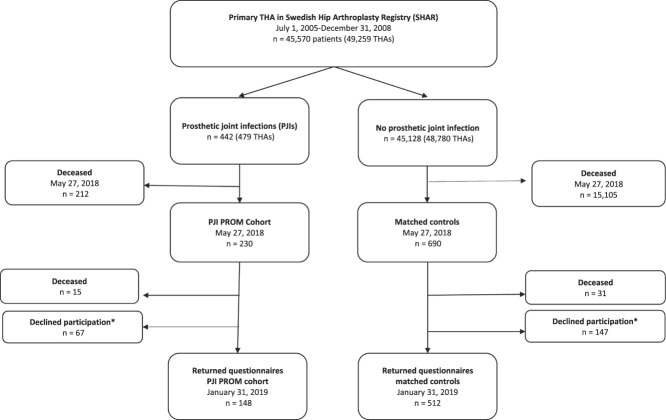
Methods: This study included 442 patients with a PJI after primary THA, from a previously published national study, including all patients with a THA performed from 2005 to 2008 in Sweden (n = 45,570) recruited from the Swedish Hip Arthroplasty Registry (SHAR). Possible deep PJIs were identified in the Swedish Dispensed Drug Registry and verified by review of medical records. Mortality in patients with PJI was compared with the remaining cohort of 45,128 patients undergoing primary THA who did not have PJI. Mortality data were retrieved from the SHAR, which in turn is updated daily from the population registry. A subgroup analysis of patients who underwent primary THA in 2008 was performed to adjust for the effect of comorbidities on mortality, as American Society of Anesthesiologists (ASA) scores became available in the SHAR at that time. For the PROM analysis, we identified three controls matched by age, gender, indication for surgery, and year of operation to each living PJI patient. A questionnaire including EQ-5D-5L, ambulatory aids, residential status, and OHS was collected from patients with PJI and controls at a mean of 11 years from the primary procedure. Apart from age and gender, we analyzed reoperation data (such as number of reoperations and surgical approach) and final prosthesis in situ to explore possible factors associated with poor PROM results.
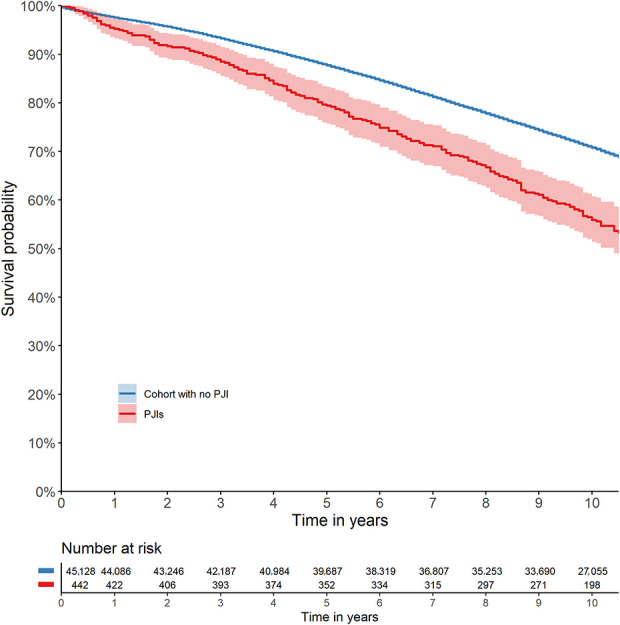
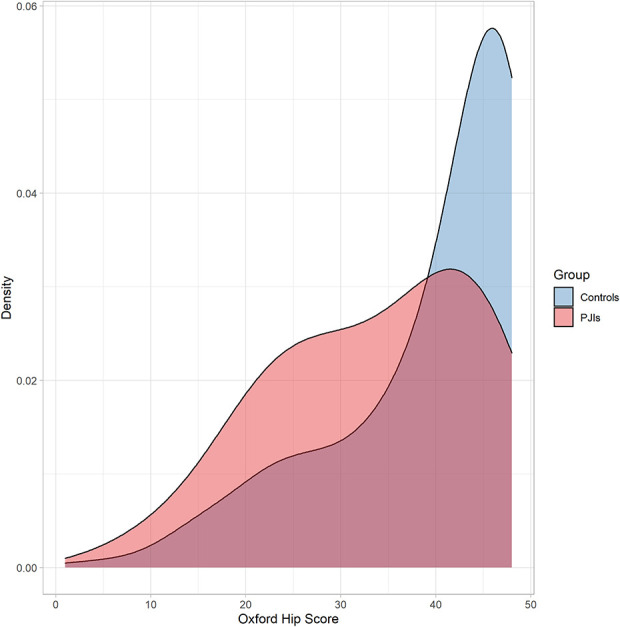
Results: After controlling for differences in sex, age, and indication for surgery, we found the all-cause 10-year mortality higher for patients with PJI (45%) compared with patients undergoing THA without PJI (29%) (odds ratio 1.4 [95% CI 1.2 to 1.6]; p < 0.001). The questionnaire, with a minimum of 10 years of follow-up, revealed a lower EQ-5D-5L index score (0.83 versus 0.94, -0.13 [95% CI -0.18 to -0.08; p < 0.001]), greater proportion of assisted living (21% versus 12%, OR 2.0 [95% CI 1.2 to 3.3]; p = 0.01), greater need of ambulatory aids (65% versus 42%, OR 3.1 [95% 2.1 to 4.8]; p < 0.001), and a lower OHS score (36 versus 44, -5.9 [-7.7 to -4.0]; p < 0.001) for patients with PJI than for matched controls. Factors associated with lower OHS score for patients with PJI were three or more reoperations (-8.0 [95% CI -13.0 to -3.2]; p = 0.01) and a direct lateral approach used at revision surgery compared with a posterior approach (-4.3 [95% CI -7.7 to -0.9]; p = 0.01).
Conclusion: In this study, we found that PJI after THA has a negative impact on mortality, long-term health-related quality of life, and hip function. Furthermore, the subgroup analysis showed that modifiable factors such as the number of reoperations and surgical approach are associated with poorer hip function. This emphasizes the importance of prompt, proper initial treatment to reduce repeated surgery to minimize the negative long-term effects of hip PJI.
Level of evidence: Level III, therapeutic study.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: What Are the Long-term Outcomes of Mortality, Quality of Life, and Hip Function after Prosthetic Joint Infection of the Hip? A 10-year Follow-up from Sweden.Clin Orthop Relat Res. 2021 Oct 1;479(10):2214-2215. doi: 10.1097/CORR.0000000000001965. Clin Orthop Relat Res. 2021. PMID: 34477573 Free PMC article. No abstract available.
References
-
- Aboltins CA, Berdal JE, Casas F, et al. Hip and knee section, prevention, antimicrobials (systemic): proceedings of international consensus on orthopedic infections. J Arthroplasty. 2019;34:S279-S288. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
