

Exploratory analysis of the effect of helminth infection on the immunogenicity and efficacy of the asexual blood-stage malaria vaccine candidate GMZ2
- PMID: 34061838
- PMCID: PMC8195366
- DOI: 10.1371/journal.pntd.0009361
Exploratory analysis of the effect of helminth infection on the immunogenicity and efficacy of the asexual blood-stage malaria vaccine candidate GMZ2
Abstract
Background: Helminths can modulate the host immune response to Plasmodium falciparum and can therefore affect the risk of clinical malaria. We assessed here the effect of helminth infections on both the immunogenicity and efficacy of the GMZ2 malaria vaccine candidate, a recombinant protein consisting of conserved domains of GLURP and MSP3, two asexual blood-stage antigens of P. falciparum. Controlled human malaria infection (CHMI) was used to assess the efficacy of the vaccine.
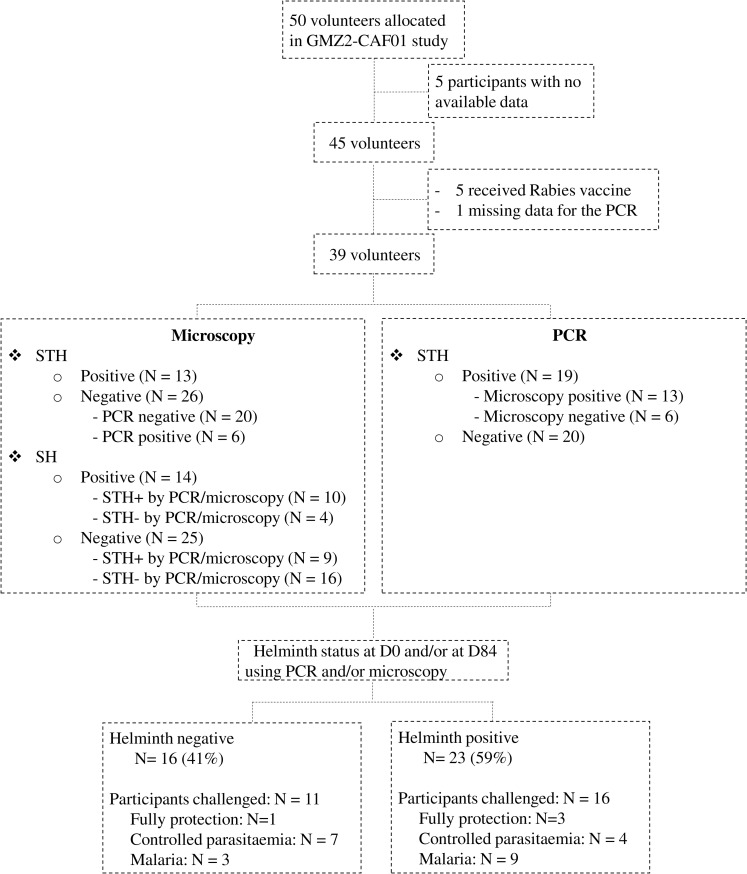
Methodology: In a randomized, double-blind Phase I clinical trial, fifty, healthy, lifelong malaria-exposed adult volunteers received three doses of GMZ2 adjuvanted with either Cationic Adjuvant Formulation (CAF) 01 or Alhydrogel, or a control vaccine (Rabies) on days (D) 0, D28 and D56, followed by direct venous inoculation (DVI) of 3,200 P. falciparum sporozoites (PfSPZ Challenge) approximately 13 weeks after last vaccination to assess vaccine efficacy. Participants were followed-up on a daily basis with clinical examinations and thick blood smears to monitor P. falciparum parasitemia for 35 days. Malaria was defined as the presence of P. falciparum parasites in the blood associated with at least one symptom that can be associated to malaria over 35 days following DVI of PfSPZ Challenge. Soil-transmitted helminth (STH) infection was assessed by microscopy and by polymerase chain reaction (PCR) on stool, and Schistosoma infection was assessed by microscopy on urine. Participants were considered as infected if positive for any helminth either by PCR and/or microscopy at D0 and/or at D84 (Helm+) and were classified as mono-infection or co-infection. Total vaccine-specific IgG concentrations assessed on D84 were analysed as immunogenicity outcome.
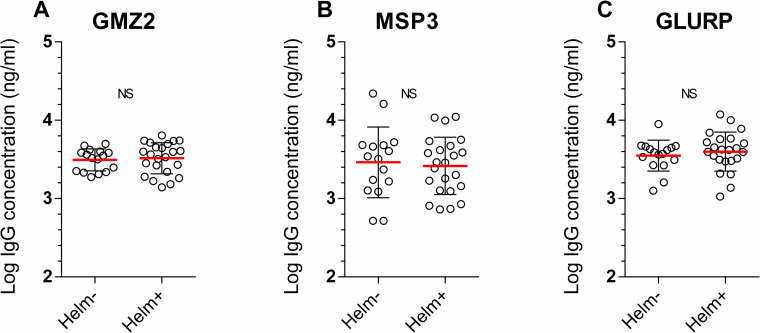
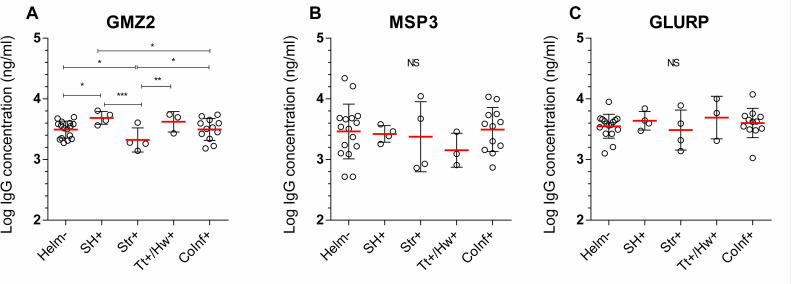
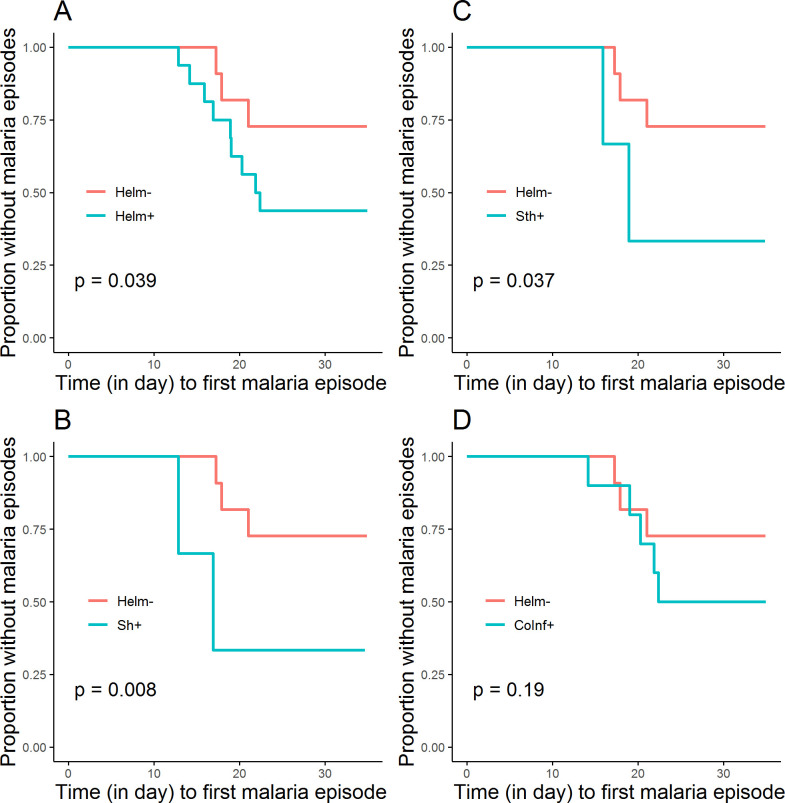
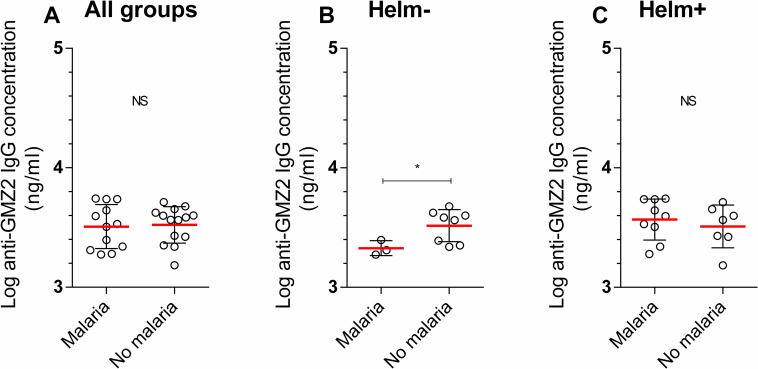
Main findings: The helminth in mono-infection, particularly Schistosoma haematobium and STH were significantly associated with earlier malaria episodes following CHMI, while no association was found in case of coinfection. In further analyses, the anti-GMZ2 IgG concentration on D84 was significantly higher in the S. haematobium-infected and significantly lower in the Strongyloides stercoralis-infected groups, compared to helminth-negative volunteers. Interesting, in the absence of helminth infection, a high anti-GMZ2 IgG concentration on D84 was significantly associated with protection against malaria.
Conclusions: Our results suggest that helminth infection may reduce naturally acquired and vaccine-induced protection against malaria. Vaccine-specific antibody concentrations on D84 may be associated with protection in participants with no helminth infection. These results suggest that helminth infection affect malaria vaccine immunogenicity and efficacy in helminth endemic countries.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Controlled Human Malaria Infection of Healthy Adults With Lifelong Malaria Exposure to Assess Safety, Immunogenicity, and Efficacy of the Asexual Blood Stage Malaria Vaccine Candidate GMZ2.Clin Infect Dis. 2019 Sep 27;69(8):1377-1384. doi: 10.1093/cid/ciy1087. Clin Infect Dis. 2019. PMID: 30561539 Free PMC article. Clinical Trial.
-
Effect of immune regulatory pathways after immunization with GMZ2 malaria vaccine candidate in healthy lifelong malaria-exposed adults.Vaccine. 2020 Jun 2;38(27):4263-4272. doi: 10.1016/j.vaccine.2020.04.046. Epub 2020 May 5. Vaccine. 2020. PMID: 32386747 Free PMC article. Clinical Trial.
-
Effect of hookworm infection and anthelmintic treatment on naturally acquired antibody responses against the GMZ2 malaria vaccine candidate and constituent antigens.BMC Infect Dis. 2021 Apr 8;21(1):332. doi: 10.1186/s12879-021-06027-5. BMC Infect Dis. 2021. PMID: 33832450 Free PMC article.
-
The GMZ2 malaria vaccine: from concept to efficacy in humans.Expert Rev Vaccines. 2017 Sep;16(9):907-917. doi: 10.1080/14760584.2017.1355246. Epub 2017 Jul 21. Expert Rev Vaccines. 2017. PMID: 28699823 Review.
-
Malaria and helminth co-infections in children living in endemic countries: A systematic review with meta-analysis.PLoS Negl Trop Dis. 2021 Feb 18;15(2):e0009138. doi: 10.1371/journal.pntd.0009138. eCollection 2021 Feb. PLoS Negl Trop Dis. 2021. PMID: 33600494 Free PMC article.
Cited by
-
Humoral antimalaria immune response in Nigerian children exposed to helminth and malaria parasites.Front Immunol. 2022 Sep 2;13:979727. doi: 10.3389/fimmu.2022.979727. eCollection 2022. Front Immunol. 2022. PMID: 36159869 Free PMC article.
-
Immunological factors linked to geographical variation in vaccine responses.Nat Rev Immunol. 2024 Apr;24(4):250-263. doi: 10.1038/s41577-023-00941-2. Epub 2023 Sep 28. Nat Rev Immunol. 2024. PMID: 37770632 Review.
-
Prevalence of malaria and helminth infections in rural communities in northern Sierra Leone, a baseline study to inform Ebola vaccine study protocols.PLoS One. 2022 Jul 6;17(7):e0270968. doi: 10.1371/journal.pone.0270968. eCollection 2022. PLoS One. 2022. PMID: 35793331 Free PMC article.
-
Safety, Tolerability, and Parasite Clearance Kinetics in Controlled Human Malaria Infection after Direct Venous Inoculation of Plasmodium falciparum Sporozoites: A Model for Evaluating New Blood-Stage Antimalarial Drugs.Am J Trop Med Hyg. 2022 Aug 29;107(4):804-814. doi: 10.4269/ajtmh.21-1297. Print 2022 Oct 12. Am J Trop Med Hyg. 2022. PMID: 36037868 Free PMC article. Clinical Trial.
-
Monocytes/Macrophages in Helminth Infections: Key Players in Host Defence, Inflammation, and Tissue Repair.Results Probl Cell Differ. 2024;74:315-340. doi: 10.1007/978-3-031-65944-7_13. Results Probl Cell Differ. 2024. PMID: 39406912 Review.
References
-
- Courtin D, Djilali-Saiah A, Milet J, Soulard V, Gaye O, Migot-Nabias F, et al.. Schistosoma haematobium infection affects Plasmodium falciparum-specific IgG responses associated with protection against malaria. Parasite Immunol. 2011. Feb;33(2):124–31. doi: 10.1111/j.1365-3024.2010.01267.x - DOI - PubMed
-
- Ateba-Ngoa U, Jones S, Zinsou JF, Honkpehedji J, Adegnika AA, Agobe JC, et al.. Associations Between Helminth Infections, Plasmodium falciparum Parasite Carriage and Antibody Responses to Sexual and Asexual Stage Malarial Antigens. Am J Trop Med Hyg. 2016. Aug;95(2):394–400. doi: 10.4269/ajtmh.15-0703 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
