

Inequities in access to primary care among opioid recipients in Ontario, Canada: A population-based cohort study
- PMID: 34061846
- PMCID: PMC8168863
- DOI: 10.1371/journal.pmed.1003631
Inequities in access to primary care among opioid recipients in Ontario, Canada: A population-based cohort study
Abstract
Background: Stigma and high-care needs can present barriers to the provision of high-quality primary care for people with opioid use disorder (OUD) and those prescribed opioids for chronic pain. We explored the likelihood of securing a new primary care provider (PCP) among people with varying histories of opioid use who had recently lost access to their PCP.
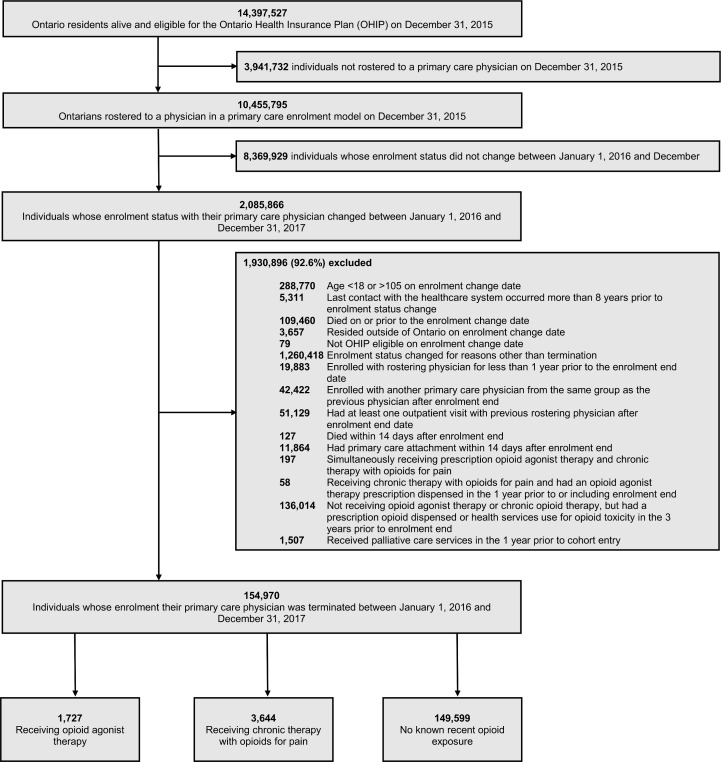
Methods and findings: We conducted a retrospective cohort study using linked administrative data among residents of Ontario, Canada whose enrolment with a physician practicing in a primary care enrolment model (PEM) was terminated between January 2016 and December 2017. We assigned individuals to 3 groups based upon their opioid use on the date enrolment ended: long-term opioid pain therapy (OPT), opioid agonist therapy (OAT), or no opioid. We fit multivariable models assessing the primary outcome of primary care reattachment within 1 year, adjusting for demographic characteristics, clinical comorbidities, and health services utilization. Secondary outcomes included rates of emergency department (ED) visits and opioid toxicity events. Among 154,970 Ontarians who lost their PCP, 1,727 (1.1%) were OAT recipients, 3,644 (2.4%) were receiving long-term OPT, and 149,599 (96.5%) had no recent prescription opioid exposure. In general, OAT recipients were younger (median age 36) than those receiving long-term OPT (59 years) and those with no recent prescription opioid exposure (44 years). In all exposure groups, the majority of individuals had their enrolment terminated by their physician (range 78.1% to 88.8%). In the primary analysis, as compared to those not receiving opioids, OAT recipients were significantly less likely to find a PCP within 1 year (adjusted hazard ratio [aHR] 0.55, 95% confidence interval [CI] 0.50 to 0.61, p < 0.0001). We observed no significant difference between long-term OPT and opioid unexposed individuals (aHR 0.96; 95% CI 0.92 to 1.01, p = 0.12). In our secondary analysis comparing the period of PCP loss to the year prior, we found that rates of ED visits were elevated among people not receiving opioids (adjusted rate ratio (aRR) 1.20, 95% CI 1.18 to 1.22, p < 0.0001) and people receiving long-term OPT (aRR 1.37, 95% CI 1.28 to 1.48, p < 0.0001). We found no such increase among OAT recipients, and no significant increase in opioid toxicity events in the period following provider loss for any exposure group. The main limitation of our findings relates to their generalizability outside of PEMs and in jurisdictions with different financial incentives incorporated into primary care provision.
Conclusions: In this study, we observed gaps in access to primary care among people who receive prescription opioids, particularly among OAT recipients. Ongoing efforts are needed to address the stigma, discrimination, and financial disincentives that may introduce barriers to the healthcare system, and to facilitate access to high-quality, consistent primary care services for chronic pain patients and those with OUD.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests to report: TG and RG have received grant funding from the Ontario Ministry of Health and CIHR. RG serves as a CIHR Scientific Director. DNJ is an unpaid member of Physicians for Responsible Opioid Prescribing (PROP). He is also a member of the American College of Medical Toxicology. Both groups have publicly available positions on this issue. He has received payment for lectures and medicolegal opinions regarding the safety and effectiveness of analgesics, including opioids. MMM has received honoraria for attending Advisory Board meetings for NovoNordisk and Neurocrine Biosciences.
Figures
Similar articles
-
Discontinuation and tapering of prescribed opioids and risk of overdose among people on long-term opioid therapy for pain with and without opioid use disorder in British Columbia, Canada: A retrospective cohort study.PLoS Med. 2022 Dec 1;19(12):e1004123. doi: 10.1371/journal.pmed.1004123. eCollection 2022 Dec. PLoS Med. 2022. PMID: 36454732 Free PMC article.
-
Hospital and physician-based mental healthcare during 12 months of opioid agonist treatment for opioid use disorder: Exploring costs and factors associated with acute care.PLoS One. 2025 Jan 8;20(1):e0314296. doi: 10.1371/journal.pone.0314296. eCollection 2025. PLoS One. 2025. PMID: 39775273 Free PMC article.
-
Trends in prescription opioid use and dose trajectories before opioid use disorder or overdose in US adults from 2006 to 2016: A cross-sectional study.PLoS Med. 2019 Nov 5;16(11):e1002941. doi: 10.1371/journal.pmed.1002941. eCollection 2019 Nov. PLoS Med. 2019. PMID: 31689302 Free PMC article.
-
[Changes in prescriptions on opioids in primary health care during the years 2008-2017].Laeknabladid. 2021 Oct;107(10):455-459. doi: 10.17992/lbl.2021.10.654. Laeknabladid. 2021. PMID: 34585671 Review. Icelandic.
-
Strategies to Identify Patient Risks of Prescription Opioid Addiction When Initiating Opioids for Pain: A Systematic Review.JAMA Netw Open. 2019 May 3;2(5):e193365. doi: 10.1001/jamanetworkopen.2019.3365. JAMA Netw Open. 2019. PMID: 31050783 Free PMC article.
Cited by
-
Designed for simplicity, used for complexity: The systemic pressures shaping walk-in clinic practices and outcomes.PLoS One. 2025 Jun 9;20(6):e0325793. doi: 10.1371/journal.pone.0325793. eCollection 2025. PLoS One. 2025. PMID: 40489477 Free PMC article.
-
Examining Access to Primary Care for People With Opioid Use Disorder in Ontario, Canada: A Randomized Clinical Trial.JAMA Netw Open. 2022 Sep 1;5(9):e2233659. doi: 10.1001/jamanetworkopen.2022.33659. JAMA Netw Open. 2022. PMID: 36178686 Free PMC article. Clinical Trial.
-
Amphetamine-Related Emergency Department Visits in Ontario, Canada, 2003-2020.Can J Psychiatry. 2023 Nov;68(11):838-849. doi: 10.1177/07067437231158933. Epub 2023 Mar 8. Can J Psychiatry. 2023. PMID: 36891572 Free PMC article.
-
Characteristics of primary care practices by proportion of patients unvaccinated against SARS-CoV-2: a cross-sectional cohort study.CMAJ. 2024 Apr 7;196(13):E432-E440. doi: 10.1503/cmaj.230816. CMAJ. 2024. PMID: 38589026 Free PMC article.
-
Prenatal opioid exposure and well-child care in the first 2 years of life: population-based cohort study.Arch Dis Child. 2023 Sep;108(9):754-761. doi: 10.1136/archdischild-2022-325029. Epub 2023 Jun 12. Arch Dis Child. 2023. PMID: 37308290 Free PMC article.
References
-
- Petterson S, McNellis R, Klink K, Meyers D, Bazemore A. The state of primary care in the United States: A chartbook of facts and statistics. Washington: Robert Graham Center; 2018.
-
- Black LI, Schiller JS. State Variation in Health Care Service Utilization: United States, 2014. NCHS Data Brief. 2016;(245):1–8. Epub 2016/05/27. . - PubMed
-
- Statistics Canada. Primary Health Care Providers, 2016 2017 [January 24, 2020]. Available from: https://www150.statcan.gc.ca/n1/pub/82-625-x/2017001/article/54863-eng.htm.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
