

Hypertrophic Cardiomyopathy and Primary Restrictive Cardiomyopathy: Similarities, Differences and Phenocopies
- PMID: 34062949
- PMCID: PMC8125617
- DOI: 10.3390/jcm10091954
Hypertrophic Cardiomyopathy and Primary Restrictive Cardiomyopathy: Similarities, Differences and Phenocopies
Abstract
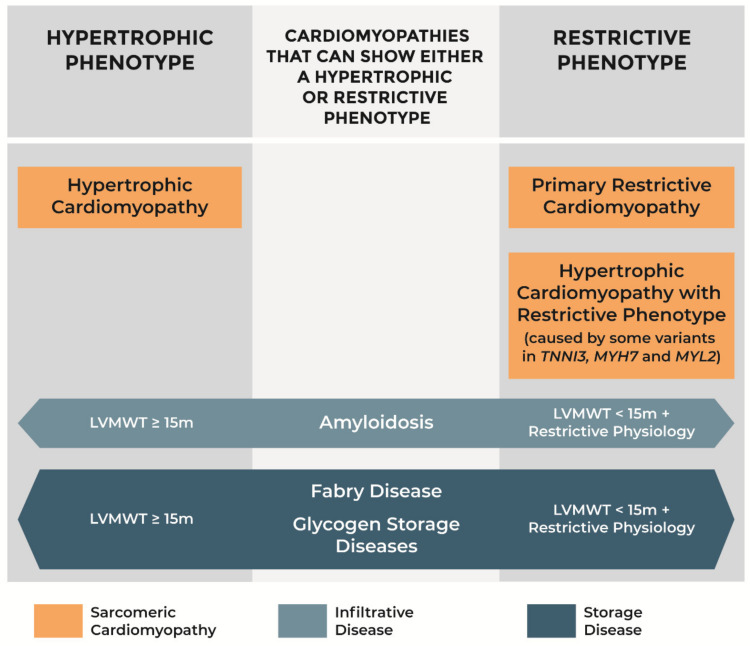
Hypertrophic cardiomyopathy (HCM) and primary restrictive cardiomyopathy (RCM) have a similar genetic background as they are both caused mainly by variants in sarcomeric genes. These "sarcomeric cardiomyopathies" also share diastolic dysfunction as the prevalent pathophysiological mechanism. Starting from the observation that patients with HCM and primary RCM may coexist in the same family, a characteristic pathophysiological profile of HCM with restrictive physiology has been recently described and supports the hypothesis that familiar forms of primary RCM may represent a part of the phenotypic spectrum of HCM rather than a different genetic cardiomyopathy. To further complicate this scenario some infiltrative (amyloidosis) and storage diseases (Fabry disease and glycogen storage diseases) may show either a hypertrophic or restrictive phenotype according to left ventricular wall thickness and filling pattern. Establishing a correct etiological diagnosis among HCM, primary RCM, and hypertrophic or restrictive phenocopies is of paramount importance for cascade family screening and therapy.
Keywords: Fabry disease; amyloidosis; cardiomyopathies; genetics; glycogen storage diseases; heart failure; hypertrophic cardiomyopathy; restrictive cardiomyopathy; restrictive physiology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Maron B.J., Towbin J.A., Thiene G., Antzelevitch C., Corrado D., Arnett D., Moss A.J., Seidman C.E., Young J.B., American Heart Association et al. Contemporary definitions and classification of the cardiomyopathies: An American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113:1807–1816. - PubMed
-
- Ommen S.R., Mital S., Burke M.A., Day S.M., Deswal A., Elliott P., Evanovich L.L., Hung J., Joglar J.A., Kantor P., et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients with Hypertrophic Cardiomyopathy: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020;142:e558–e631. - PubMed
-
- Biagini E., Spirito P., Rocchi G., Ferlito M., Rosmini S., Lai F., Lorenzini M., Terzi F., Bacchi-Reggiani L., Boriani G., et al. Prognostic Implications of the Doppler Restrictive Filling Pattern in Hypertrophic Cardiomyopathy. Am. J. Cardiol. 2009;104:1727–1731. doi: 10.1016/j.amjcard.2009.07.057. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
