

Idiopathic Intracranial Hypertension: Evaluation of Admissions and Emergency Readmissions through the Hospital Episode Statistic Dataset between 2002-2020
- PMID: 34063037
- PMCID: PMC8148005
- DOI: 10.3390/life11050417
Idiopathic Intracranial Hypertension: Evaluation of Admissions and Emergency Readmissions through the Hospital Episode Statistic Dataset between 2002-2020
Abstract
With increasing incidence and prevalence of Idiopathic intracranial hypertension in the UK, the aim of this study was to explore emerging themes in Idiopathic intracranial hypertension using the Hospital Episode Statistics dataset and to quantify recent change in hospital admissions and surgeries performed within England.
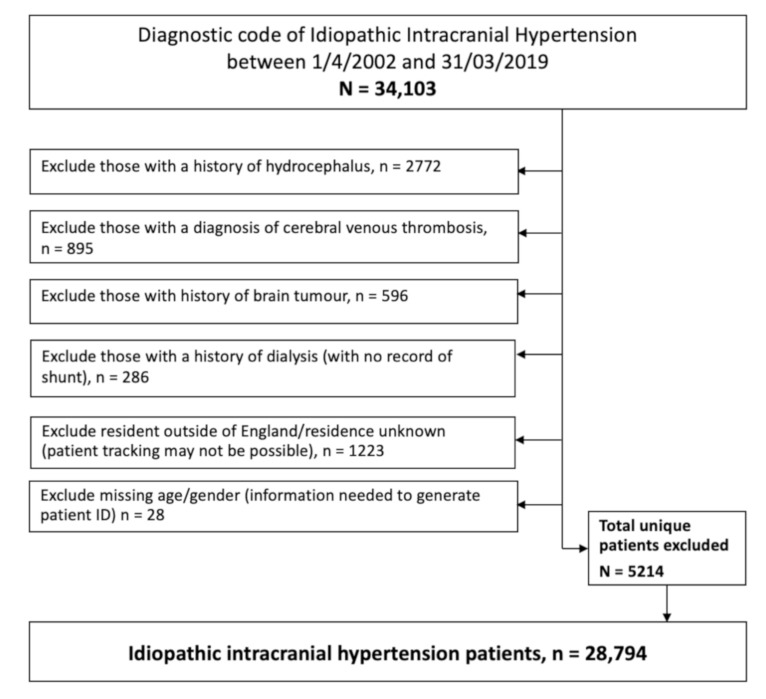
Methods: Hospital Episode Statistics national data was extracted between 1 April 2002 and 31 March 2019, and followed up until 31 March 2020. All those within England with a diagnosis of Idiopathic Intracranial Hypertension were included. Those with secondary causes of raised intracranial pressure such as tumors, hydrocephalus and cerebral venous sinus thrombosis were excluded.
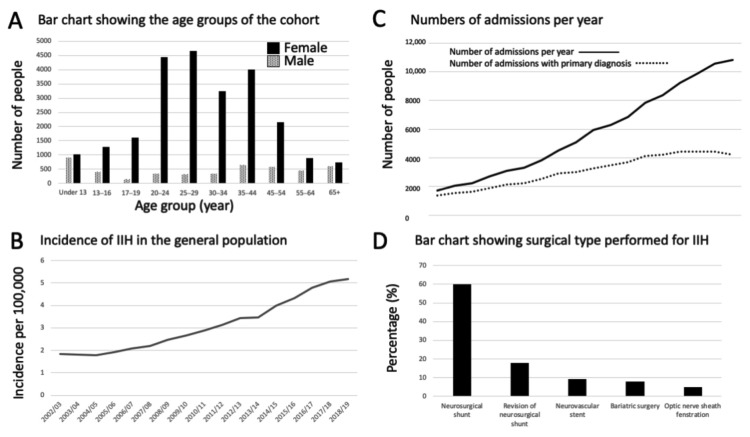
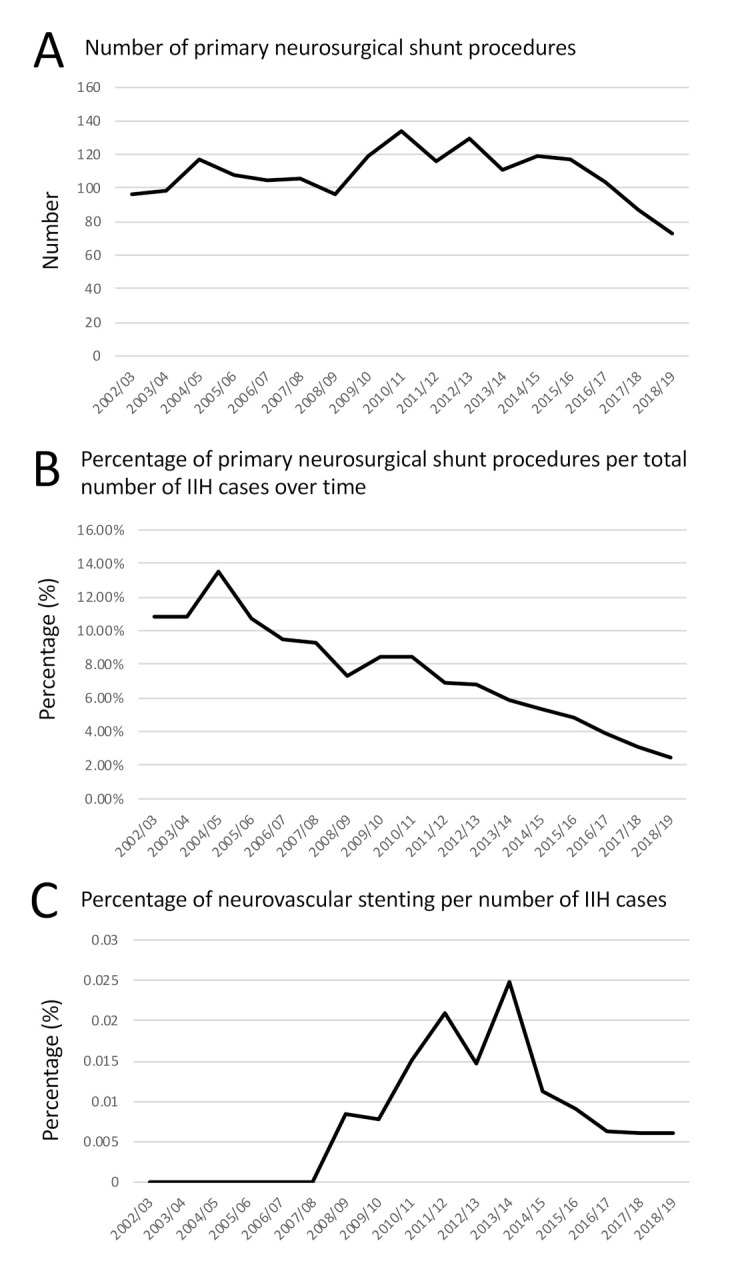
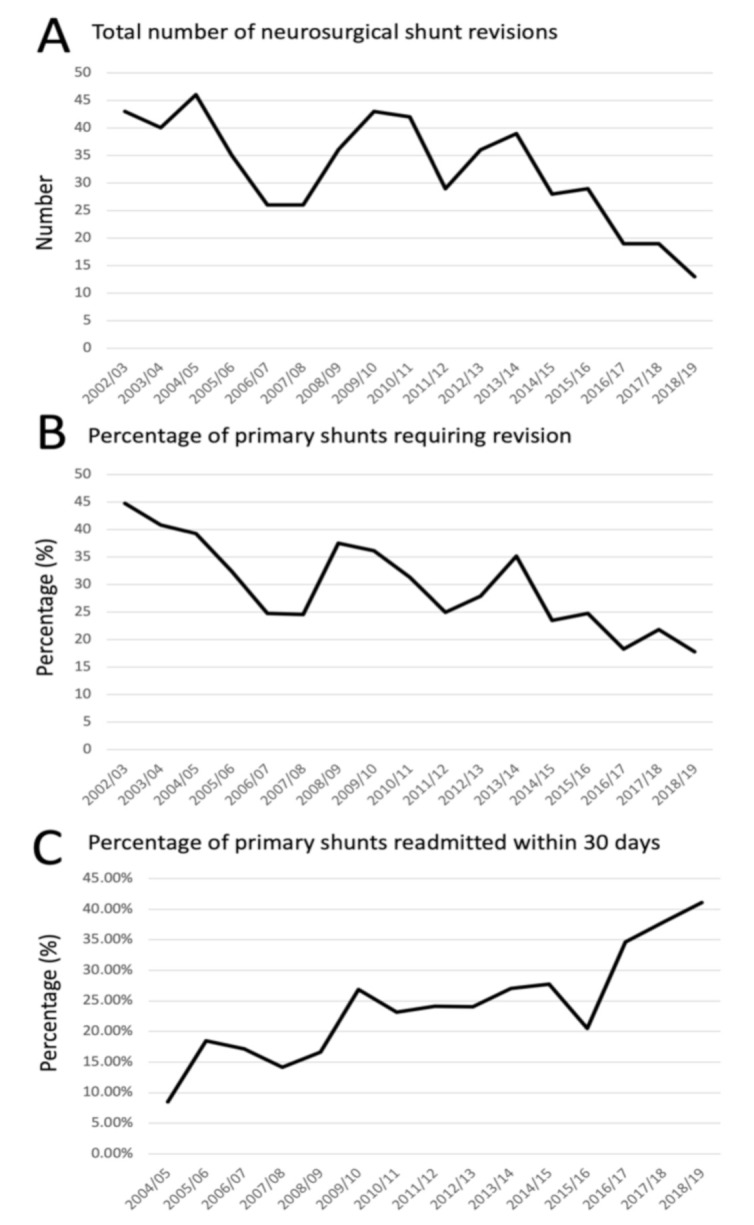
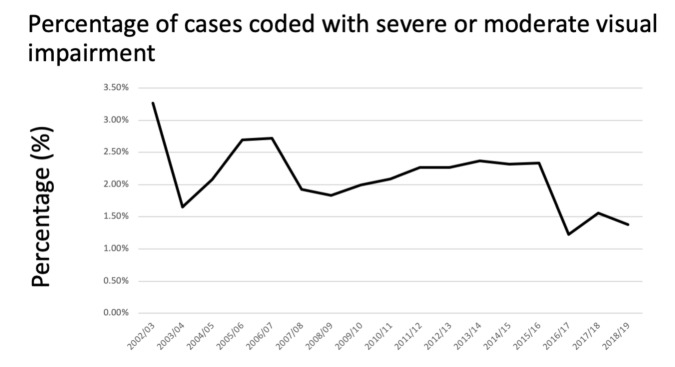
Results: 28,794 new IIH cases were diagnosed between 1 January 2002 and 31 December 2019. Incidence rose between 2002 to 2019 from 1.8 to 5.2 per 100,000 in the general population. Peak incidence occurred in females aged 25-29 years. Neurosurgical shunt was the commonest procedure performed (6.4%), followed by neovascular venous sinus stenting (1%), bariatric surgery (0.8%) and optic nerve sheath fenestration (0.5%). The portion of the total IIH population requiring a shunt fell from 10.8% in 2002/2003 to 2.46% in 2018/2019. The portion of the total IIH population requiring shunt revision also reduced over time from 4.84% in 2002/2003 to 0.44% in 2018/2019. The mean 30 days emergency readmissions for primary shunt, revision of shunt, bariatric surgery, neurovascular stent, and optic nerve sheath fenestration was 23.1%, 23.7%, 10.6%, 10.0% and 9.74%, respectively. There was a peak 30 days readmission rate following primary shunt in 2018/2019 of 41%. Recording of severe visual impairment fell to an all-time low of 1.38% in 2018/19.
Conclusions: Increased awareness of the condition, specialist surgery and expert guidance may be changing admissions and surgical trends in IIH. The high 30 readmission following primary shunt surgery for IIH requires further investigation.
Keywords: 30 days readmission; emergency; hospital episode statistic; idiopathic intracranial hypertension; neurosurgery; papilloedema; pseudotumor cerebri; revision; shunt; stent.
Conflict of interest statement
Mollan reports other Invex Therapeutics, other Heidelberg engineering during the conduct of the study; other from Chugai-Roche Ltd., other from Janssen, other from Allergan, other from Santen, other from Roche, other from Neurodiem, outside the submitted work. Professor Sinclair reports salary and stock options from Invex therapeutics, during the conduct of the study. All other authors declare no competing interests.
Figures
References
-
- Adderley N.J., Subramanian A., Nirantharakumar K., Yiangou A., Gokhale K.M., Mollan S.P., Sinclair A.J. Association between idiopathic intracranial hypertension and risk of cardiovascular diseases in women in the United Kingdom. JAMA Neurol. 2019;76:1088–1098. doi: 10.1001/jamaneurol.2019.1812. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
