

Perioperative Vascular Biomarker Profiling in Elective Surgery Patients Developing Postoperative Delirium: A Prospective Cohort Study
- PMID: 34063403
- PMCID: PMC8155907
- DOI: 10.3390/biomedicines9050553
Perioperative Vascular Biomarker Profiling in Elective Surgery Patients Developing Postoperative Delirium: A Prospective Cohort Study
Abstract
Background: Postoperative delirium (POD) ranks among the most common complications in surgical patients. Blood-based biomarkers might help identify the patient at risk. This study aimed to assess how serum biomarkers with specificity for vascular and endothelial function and for inflammation are altered, prior to or following surgery in patients who subsequently develop POD.
Methods: This was a study on a subcohort of consecutively recruited elective non-cardiac as well as cardiac surgery patients (age > 60 years) of the single-center PROPDESC trial at a German tertiary care hospital. Serum was sampled prior to and following surgery, and the samples were subjected to bead-based multiplex analysis of 17 serum proteins (IL-3, IL-8, IL-10, Cripto, CCL2, RAGE, Resistin, ANGPT2, TIE2, Thrombomodulin, Syndecan-1, E-Selectin, VCAM-1, ICAM-1, CXCL5, NSE, and uPAR). Development of POD was assessed during the first five days after surgery, using the Confusion Assessment Method for ICU (CAM-ICU), the CAM, the 4-'A's test (4AT), and the Delirium Observation Scale (DOS). Patients were considered positive if POD was detected at least once during the visitation period by any of the applied methods. Non-parametric testing, as well as propensity score matching were used for statistical analysis.
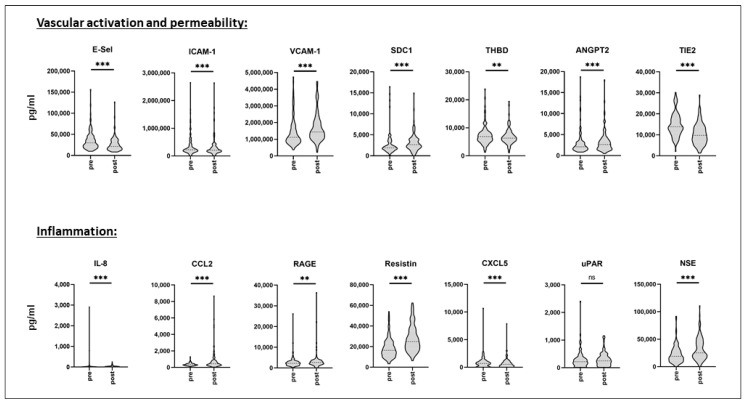
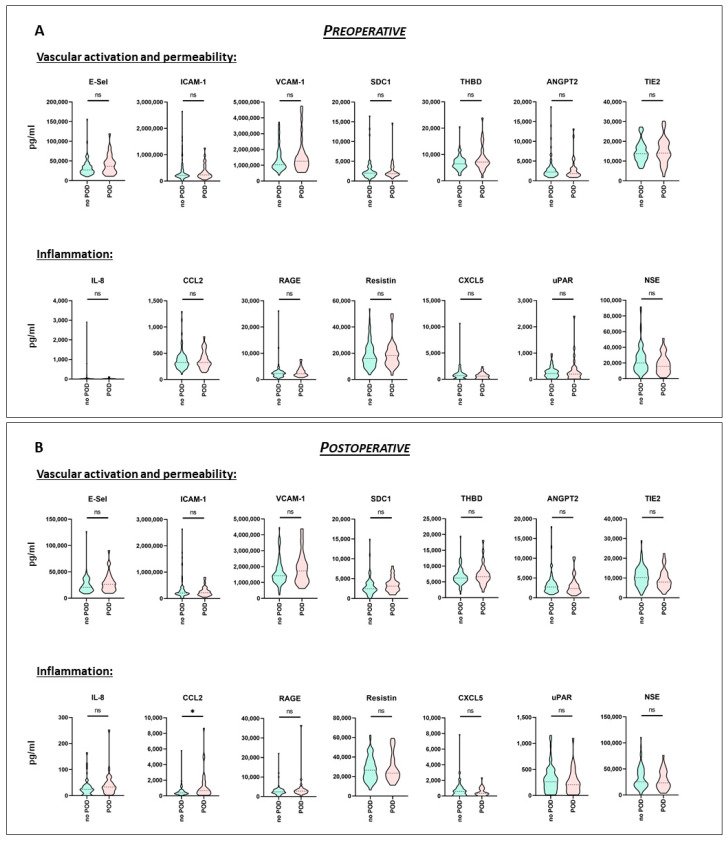
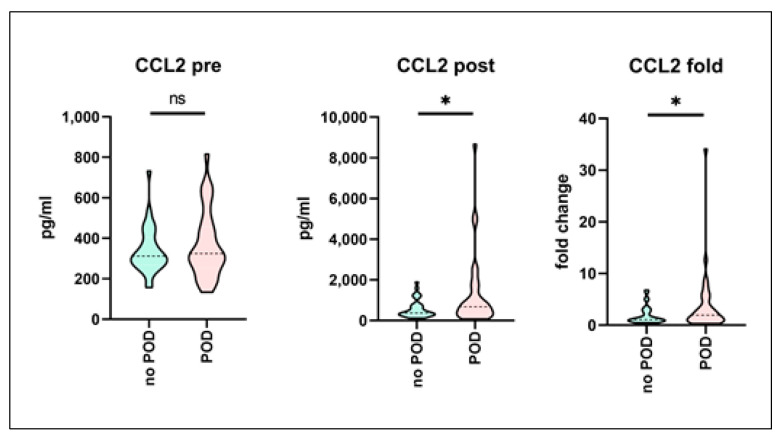
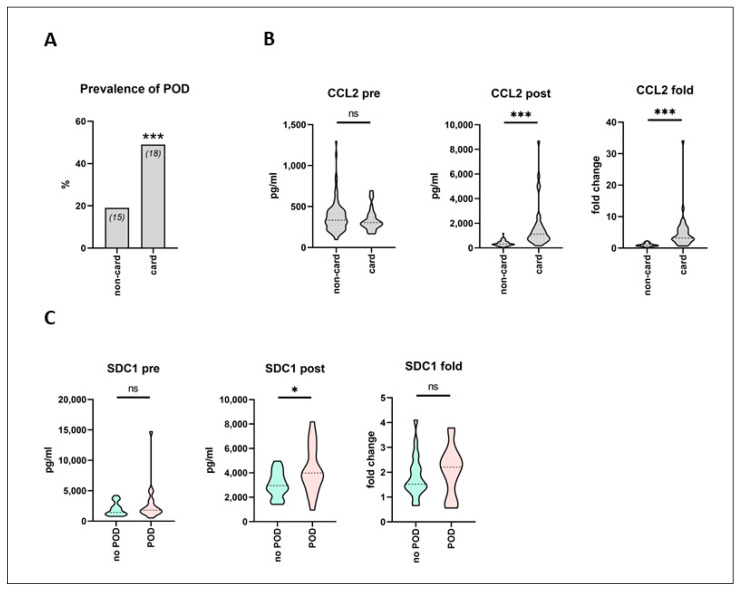
Results: A total of 118 patients were included in the final analysis; 69% underwent non-cardiac surgery, median overall patient age was 71 years, and 59% of patients were male. In the whole cohort, incidence of POD was 28%. The male gender was significantly associated with the development of POD (p = 0.0004), as well as a higher ASA status III (p = 0.04). Incidence of POD was furthermore significantly increased in cardiac surgery patients (p = 0.002). Surgery induced highly significant changes in serum levels of almost all biomarkers except uPAR. In preoperative serum samples, none of the analyzed parameters was significantly altered in subsequent POD patients. In postoperative samples, CCL2 was significantly increased by a factor of 1.75 in POD patients (p = 0.03), as compared to the no-POD cohort. Following propensity score matching, CCL2 remained the only biomarker that showed significant differences in postoperative values (p = 0.01). In cardiac surgery patients, postoperative CCL2 serum levels were more than 3.5 times higher than those following non-cardiac surgery (p < 0.0001). Moreover, after cardiac surgery, Syndecan-1 serum levels were significantly increased in POD patients, as compared to no-POD cardiac surgery patients (p = 0.04).
Conclusions: In a mixed cohort of elective non-cardiac as well as cardiac surgery patients, preoperative serum biomarker profiling with specificity for vascular dysfunction and for systemic inflammation was not indicative of subsequent POD development. Surgery-induced systemic inflammation-as evidenced by the significant increase in CCL2 release-was associated with POD, particularly following cardiac surgery. In those patients, postoperative glycocalyx injury might furthermore contribute to POD development.
Keywords: CCL2; MCP-1; biomarker; cardiac surgery; elective surgery; glycocalyx; postoperative delirium; vascular inflammation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; Arlington, VA, USA: 2013.
-
- Gleason L.J., Schmitt E.M., Kosar C.M., Tabloski P., Saczynski J.S., Robinson T.N., Cooper Z., Rogers S.O., Jones R.N., Marcantonio E.R., et al. Effect of Delirium and Other Major Complications on Outcomes After Elective Surgery in Older Adults. JAMA Surg. 2015;150:1134–1140. doi: 10.1001/jamasurg.2015.2606. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
