

Children's Preferences for Oral Dosage Forms and Their Involvement in Formulation Research via EPTRI (European Paediatric Translational Research Infrastructure)
- PMID: 34063499
- PMCID: PMC8156390
- DOI: 10.3390/pharmaceutics13050730
Children's Preferences for Oral Dosage Forms and Their Involvement in Formulation Research via EPTRI (European Paediatric Translational Research Infrastructure)
Abstract
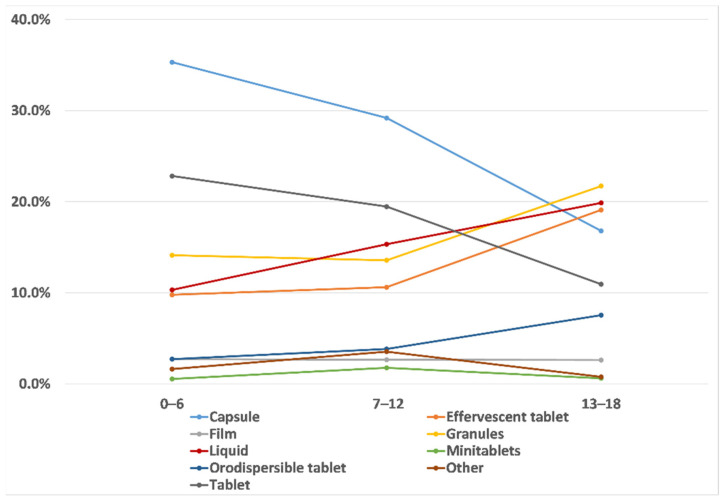
The paucity of evidence-based data on formulation characteristics preferred by the children is known to limit the design of tailored paediatric dosage forms. The European Paediatric Translational Research Infrastructure (EPTRI) commissioned a study to evaluate children's dosage forms perceived preferences in some European countries and explore the feasibility of using the young persons advisory groups (YPAGs) to involve children in formulation research. An online, age-adapted survey was developed and translated into six languages. The survey link was disseminated across seven European countries: Albania, Italy, the Netherlands, and Dutch-speaking part of Belgium, Romania, Spain, and the United Kingdom. Respondents' (n = 1172) perceived preferences for oral dosage forms primarily differed based on age, health status, and experience. Conventional dosage forms, i.e., liquid (35%), tablets (19%), and capsules (14%), were the most selected. Liquid was widely selected by children less than 12 years and by those healthy and taking medicines rarely. Monolithic solid forms were mostly chosen by adolescents and by children with a chronic disease taking medicines frequently. There was a clear lack of familiarity with more novel dosage forms (e.g., orodispersible films and granules). Noteworthy, granules were not appreciated, particularly by adolescents (52.8%). To rationalise the creation of paediatric formulations, it is important to involve children as active stakeholders and to apply tools assessing children's perspectives on medicines to inform acceptable dosage form development from the start.
Keywords: EPTRI; medicines acceptability; oral dosage forms; paediatric formulations; patient-centric research.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







References
-
- Ranmal S.R., Cram A., Tuleu C. Age-Appropriate and Acceptable Paediatric Dosage Forms: Insights into End-User Perceptions, Preferences and Practices from the Children’s Acceptability of Oral Formulations (CALF) Study. Int. J. Pharm. 2016;514:296–307. doi: 10.1016/j.ijpharm.2016.07.054. - DOI - PubMed
-
- European Medicines Agency Guideline on Pharmaceutical Development of Medicines for Paediatric Use. [(accessed on 8 June 2020)];2013 Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-ph....
-
- Lallemant M. Module 5: Acceptability. [(accessed on 9 June 2020)]; Available online: https://www.who.int/hiv/pub/5.pdf.
Grants and funding
LinkOut - more resources
Full Text Sources
