

A Prospective Feasibility Trial to Challenge Patient-Derived Pancreatic Cancer Organoids in Predicting Treatment Response
- PMID: 34064221
- PMCID: PMC8196829
- DOI: 10.3390/cancers13112539
A Prospective Feasibility Trial to Challenge Patient-Derived Pancreatic Cancer Organoids in Predicting Treatment Response
Abstract
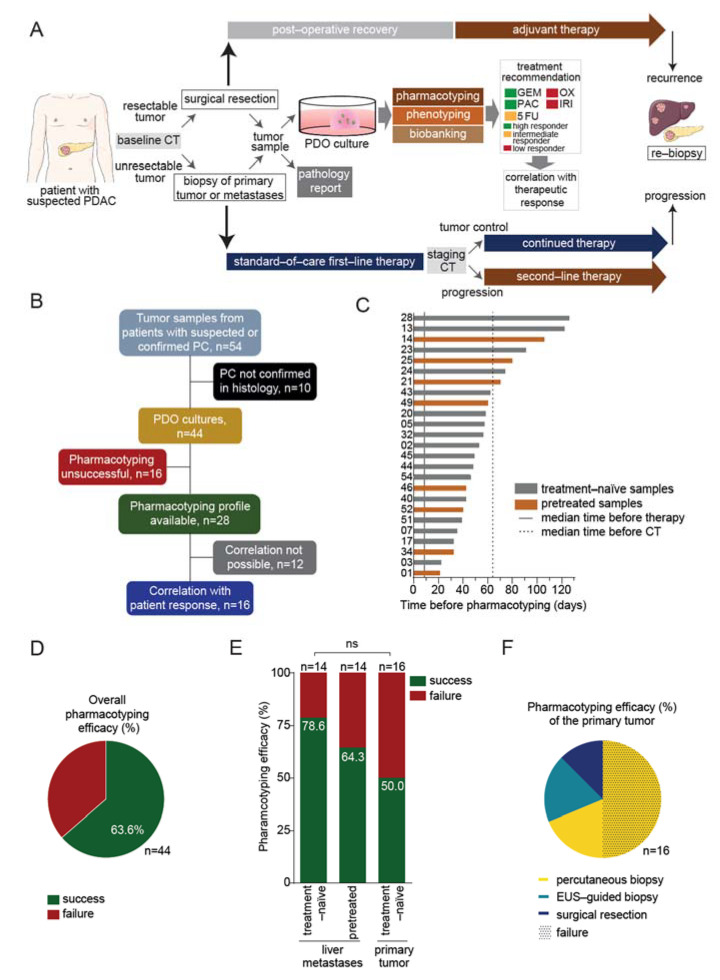
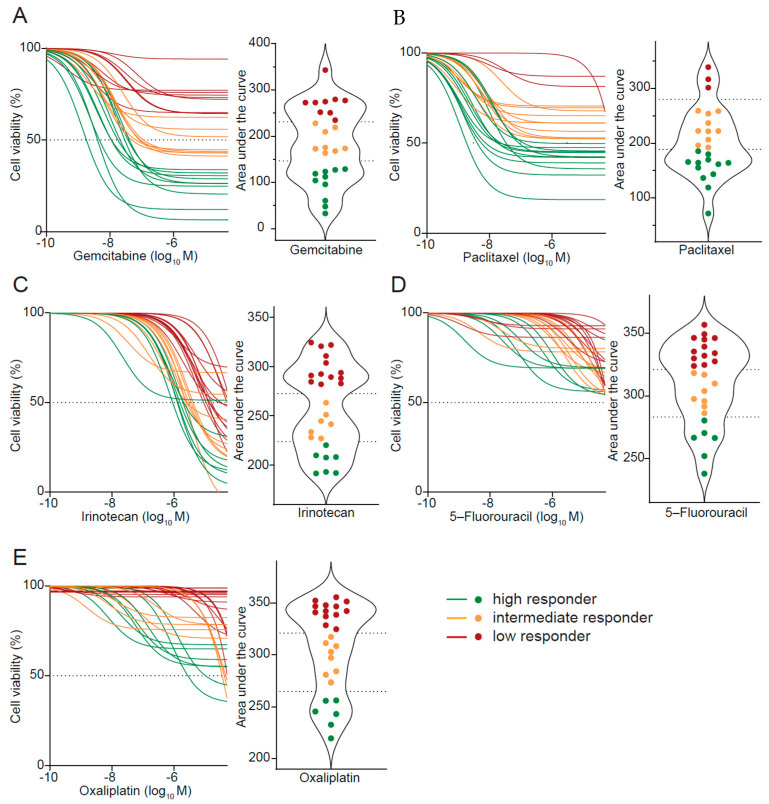
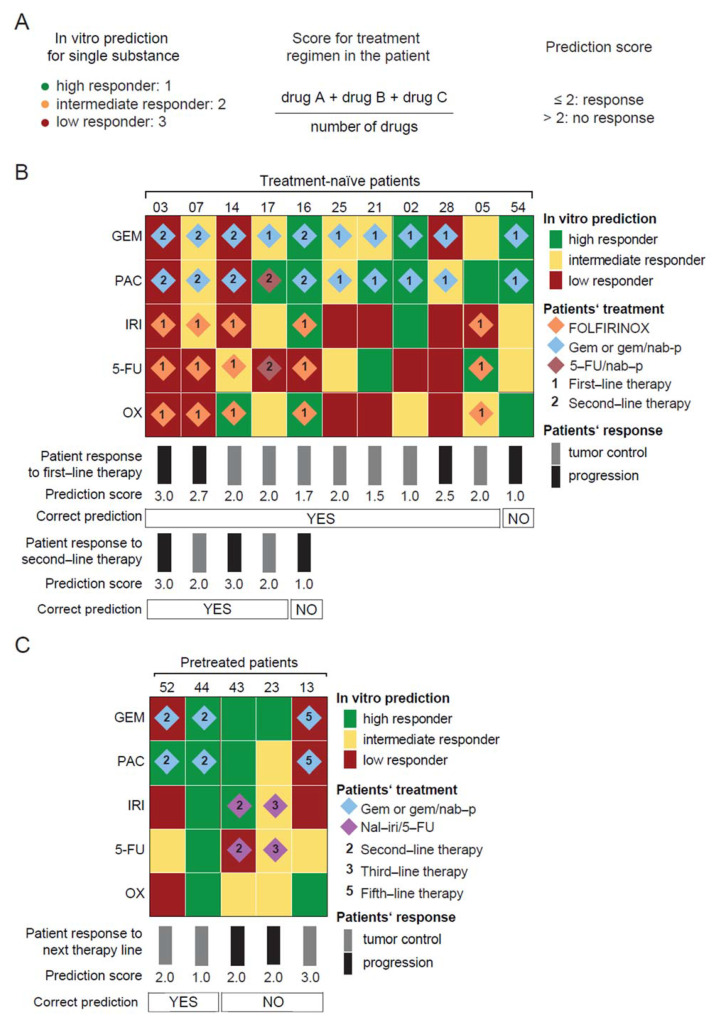
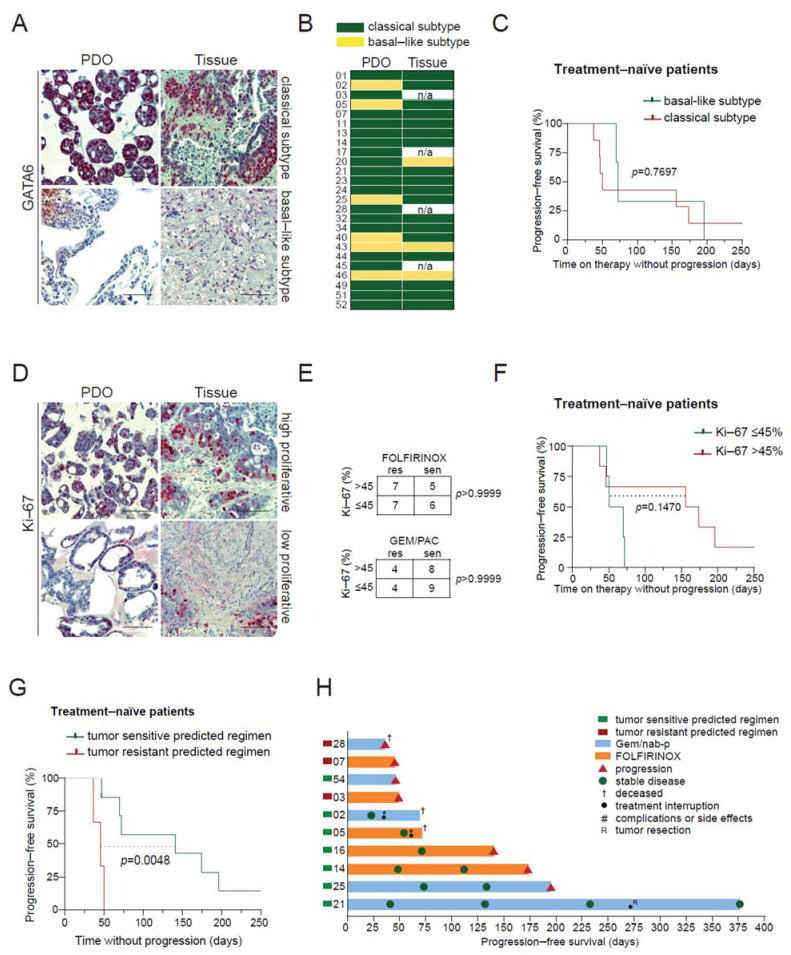
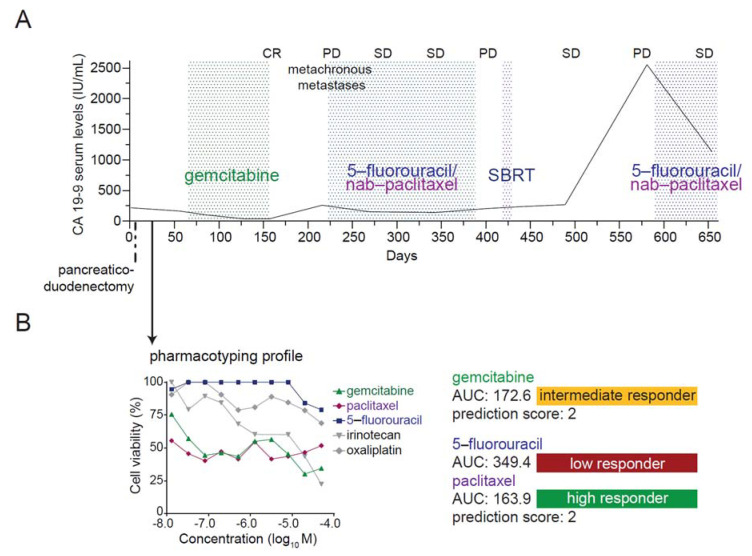
Real-time isolation, propagation, and pharmacotyping of patient-derived pancreatic cancer organoids (PDOs) may enable treatment response prediction and personalization of pancreatic cancer (PC) therapy. In our methodology, PDOs are isolated from 54 patients with suspected or confirmed PC in the framework of a prospective feasibility trial. The drug response of single agents is determined by a viability assay. Areas under the curves (AUC) are clustered for each drug, and a prediction score is developed for combined regimens. Pharmacotyping profiles are obtained from 28 PDOs (efficacy 63.6%) after a median of 53 days (range 21-126 days). PDOs exhibit heterogeneous responses to the standard-of-care drugs, and are classified into high, intermediate, or low responder categories. Our developed prediction model allows a successful response prediction in treatment-naïve patients with an accuracy of 91.1% for first-line and 80.0% for second-line regimens, respectively. The power of prediction declines in pretreated patients (accuracy 40.0%), particularly with more than one prior line of chemotherapy. Progression-free survival (PFS) is significantly longer in previously treatment-naïve patients receiving a predicted tumor sensitive compared to a predicted tumor resistant regimen (mPFS 141 vs. 46 days; p = 0.0048). In conclusion, generation and pharmacotyping of PDOs is feasible in clinical routine and may provide substantial benefit.
Keywords: drug response prediction; organoids; pancreatic cancer; personalized medicine; pharmacotyping.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Pishvaian M.J., Blais E.M., Brody J.R., Lyons E., DeArbeloa P., Hendifar A., Mikhail S., Chung V., Sahai V., Sohal D.P.S., et al. Overall survival in patients with pancreatic cancer receiving matched therapies following molecular profiling: A retrospective analysis of the Know Your Tumor registry trial. Lancet Oncol. 2020;21:508–518. doi: 10.1016/S1470-2045(20)30074-7. - DOI - PMC - PubMed
-
- Bachet J.B., Mitry E., Lievre A., Lepere C., Vaillant J.N., Declety G., Parlier H., Emile J.F., Julie C., Rougier P. Second- and third-line chemotherapy in patients with metastatic pancreatic adenocarcinoma: Feasibility and potential benefits in a retrospective series of 117 patients. Gastroentérol. Clin. Biol. 2009;33:1036–1044. doi: 10.1016/j.gcb.2009.03.017. - DOI - PubMed
LinkOut - more resources
Full Text Sources
