

The Spectrum of COVID-19-Associated Myocarditis: A Patient-Tailored Multidisciplinary Approach
- PMID: 34064463
- PMCID: PMC8124580
- DOI: 10.3390/jcm10091974
The Spectrum of COVID-19-Associated Myocarditis: A Patient-Tailored Multidisciplinary Approach
Abstract
Background: Myocarditis lacks systematic characterization in COVID-19 patients.
Methods: We enrolled consecutive patients with newly diagnosed myocarditis in the context of COVID-19 infection. Diagnostic and treatment strategies were driven by a dedicated multidisciplinary disease unit for myocarditis. Multimodal outcomes were assessed during prospective follow-up.
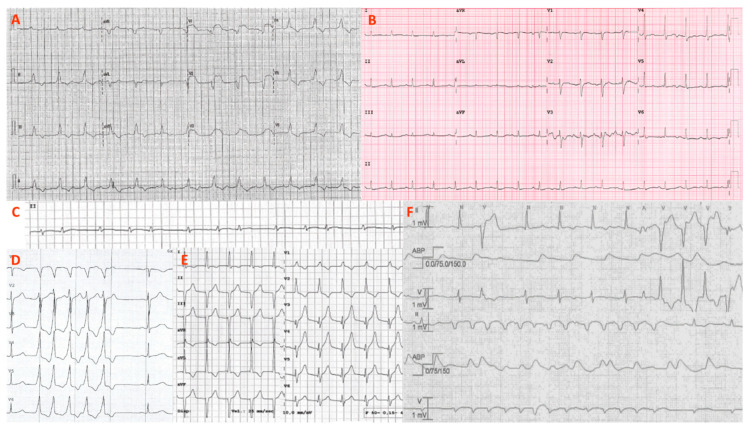
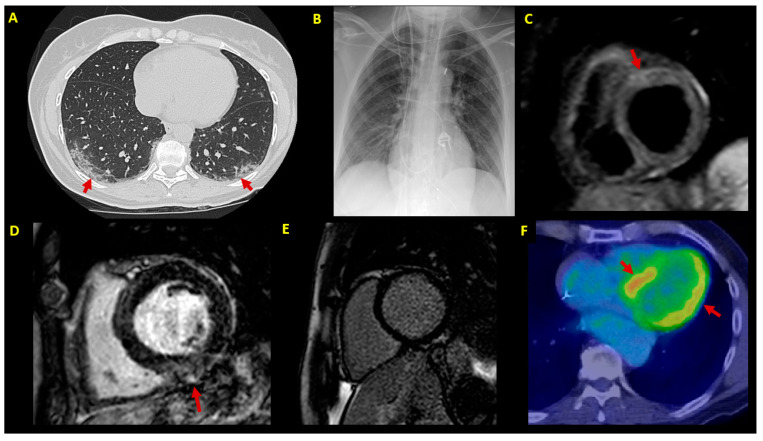
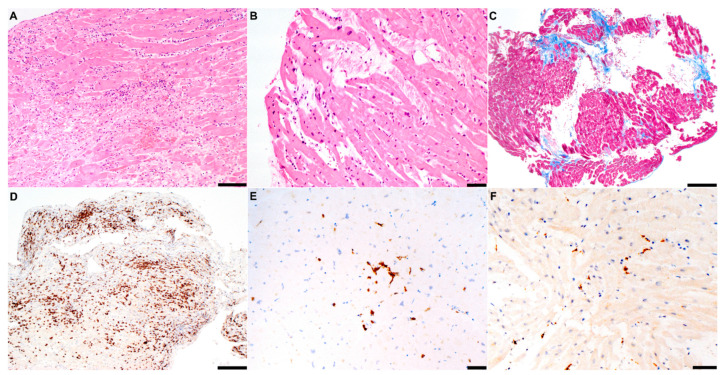
Results: Seven consecutive patients (57% males, age 51 ± 9 y) with acute COVID-19 infection received a de novo diagnosis of myocarditis. Endomyocardial biopsy was of choice in hemodynamically unstable patients (n = 4, mean left ventricular ejection fraction (LVEF) 25 ± 9%), whereas cardiac magnetic resonance constituted the first exam in stable patients (n = 3, mean LVEF 48 ± 10%). Polymerase chain reaction (PCR) analysis revealed an intra-myocardial SARS-CoV-2 genome in one of the six cases undergoing biopsy: in the remaining patients, myocarditis was either due to other viruses (n = 2) or virus-negative (n = 3). Hemodynamic support was needed for four unstable patients (57%), whereas a cardiac device implant was chosen in two of four cases showing ventricular arrhythmias. Medical treatment included immunosuppression (43%) and biological therapy (29%). By the 6-month median follow-up, no patient died or experienced malignant arrhythmias. However, two cases (29%) were screened for heart transplantation.
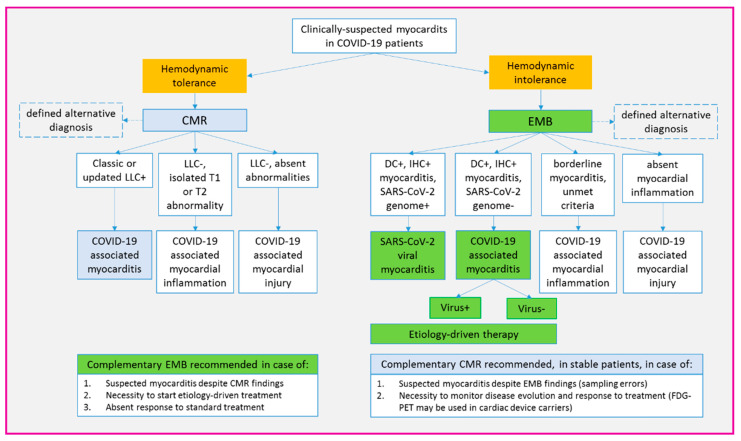
Conclusions: Myocarditis associated with acute COVID-19 infection is a spectrum of clinical manifestations and underlying etiologies. A multidisciplinary approach is the cornerstone for tailored management.
Keywords: COVID-19; SARS-CoV-2; cardiac magnetic resonance; endomyocardial biopsy; immunosuppression; inflammation; multidisciplinary; myocarditis; ventricular arrhythmias.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Tschöpe C., Ammirati E., Bozkurt B., Caforio A.L.P., Cooper L.T., Felix S.B., Hare J.M., Heidecker B., Heymans S., Hübner N., et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2020:1–25. doi: 10.1038/s41569-020-00435-x. - DOI - PMC - PubMed
-
- Peretto G., De Luca G., Campochiaro C., Palmisano A., Busnardo E., Sartorelli S., Barzaghi F., Cicalese M.P., Esposito A., Sala S. Telemedicine in myocarditis: Evolution of a mutidisciplinary "disease unit" at the time of COVID-19 pandemic. Am. Heart J. 2020;229:121–126. doi: 10.1016/j.ahj.2020.07.015. - DOI - PMC - PubMed
-
- Ferreira V.M., Schulz-Menger J., Holmvang G., Kramer C.M., Carbone I., Sechtem U., Kindermann I., Gutberlet M., Cooper L.T., Liu P., et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J. Am. Coll. Cardiol. 2018;72:3158–3176. doi: 10.1016/j.jacc.2018.09.072. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
