

Imprecise Medicine: BRCA2 Variants of Uncertain Significance (VUS), the Challenges and Benefits to Integrate a Functional Assay Workflow with Clinical Decision Rules
- PMID: 34065235
- PMCID: PMC8161351
- DOI: 10.3390/genes12050780
Imprecise Medicine: BRCA2 Variants of Uncertain Significance (VUS), the Challenges and Benefits to Integrate a Functional Assay Workflow with Clinical Decision Rules
Abstract
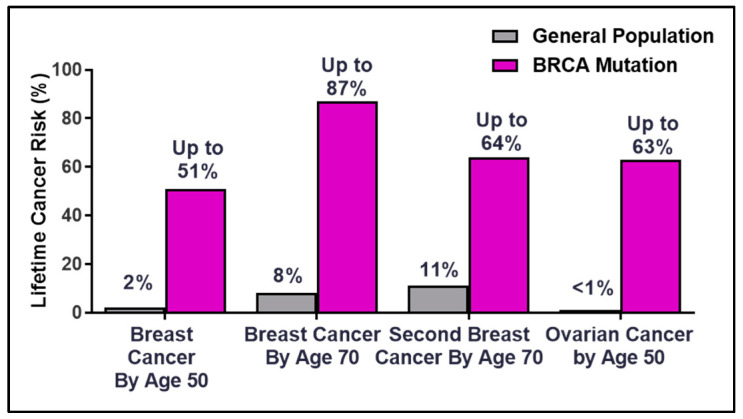
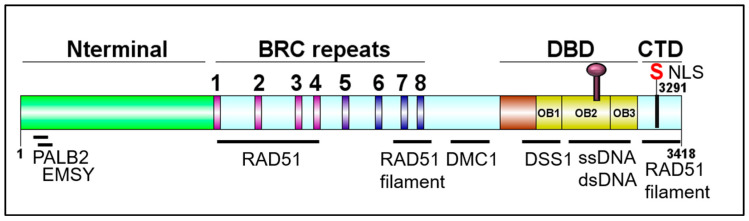
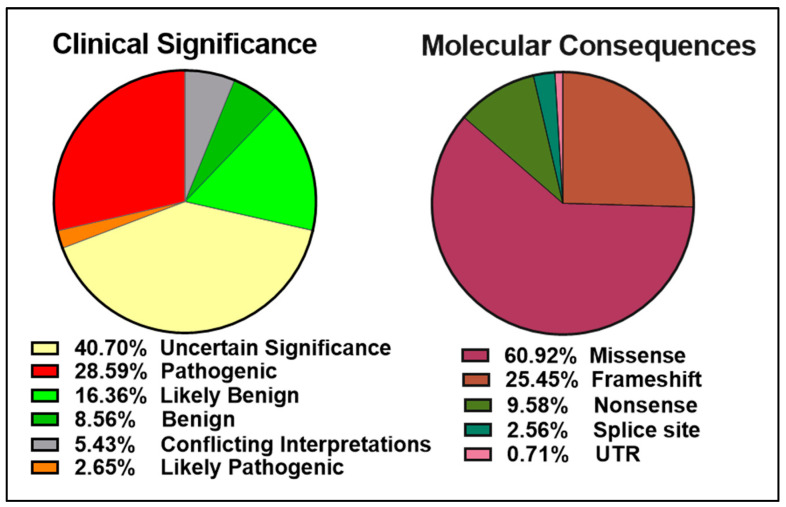
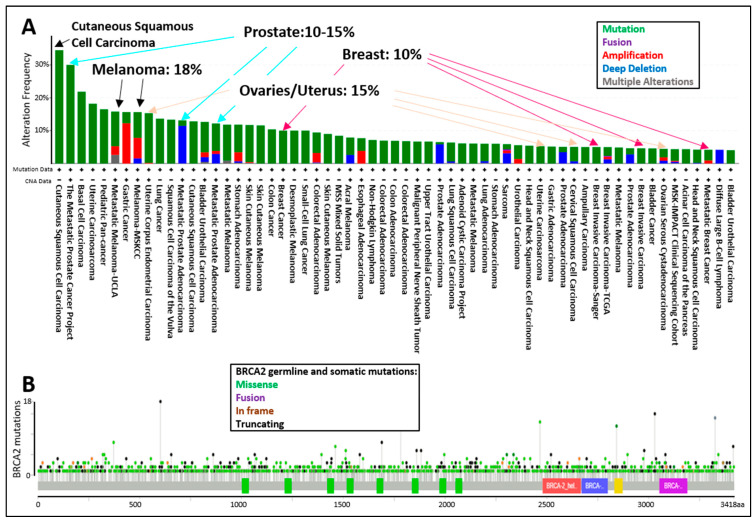
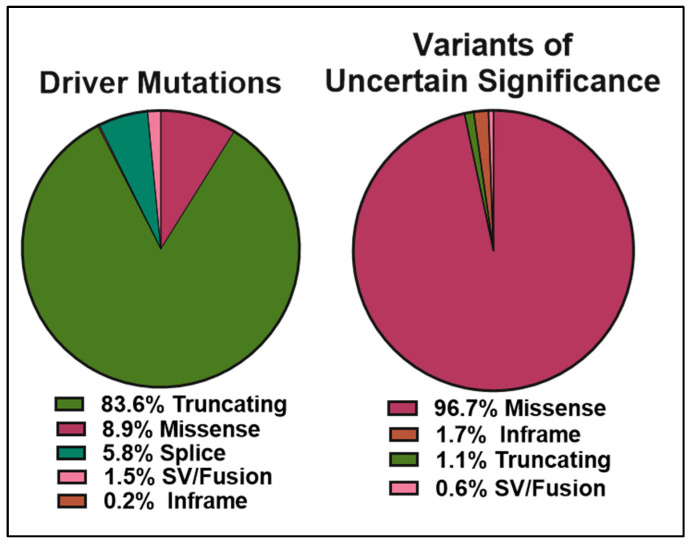
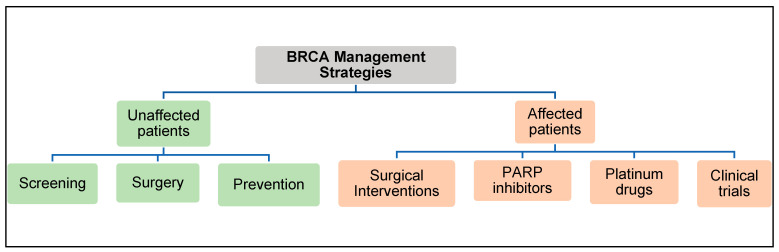
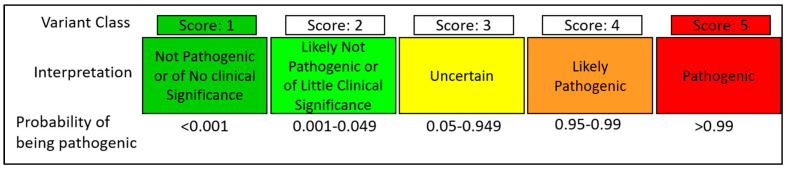
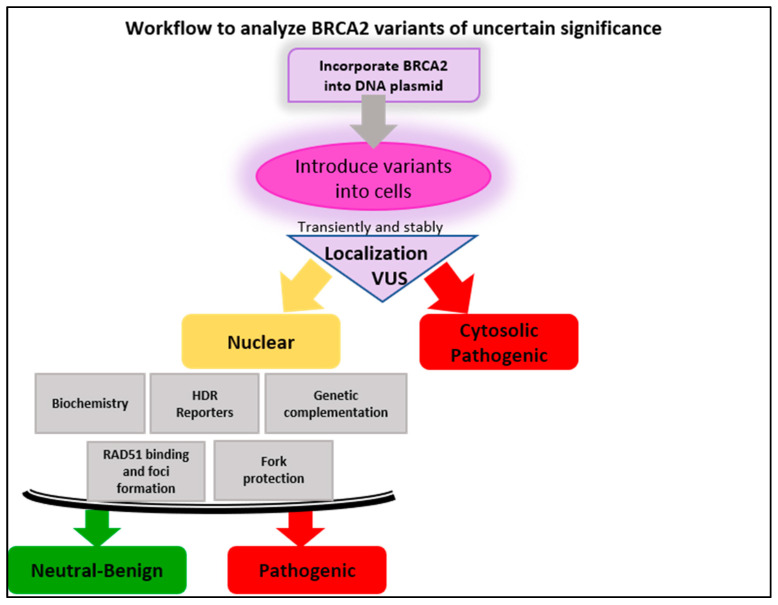
Pathological mutations in homology-directed repair (HDR) genes impact both future cancer risk and therapeutic options for patients. HDR is a high-fidelity DNA repair pathway for resolving DNA double-strand breaks throughout the genome. BRCA2 is an essential protein that mediates the loading of RAD51 onto resected DNA breaks, a key step in HDR. Germline mutations in BRCA2 are associated with an increased risk for breast, ovarian, prostate, and pancreatic cancer. Clinical findings of germline or somatic BRCA2 mutations in tumors suggest treatment with platinum agents or PARP inhibitors. However, when genetic analysis reveals a variant of uncertain significance (VUS) in the BRCA2 gene, precision medicine-based decisions become complex. VUS are genetic changes with unknown pathological impact. Current statistics indicate that between 10-20% of BRCA sequencing results are VUS, and of these, more than 50% are missense mutations. Functional assays to determine the pathological outcome of VUS are urgently needed to provide clinical guidance regarding cancer risk and treatment options. In this review, we provide a brief overview of BRCA2 functions in HDR, describe how BRCA2 VUS are currently assessed in the clinic, and how genetic and biochemical functional assays could be integrated into the clinical decision process. We suggest a multi-step workflow composed of robust and accurate functional assays to correctly evaluate the potential pathogenic or benign nature of BRCA2 VUS. Success in this precision medicine endeavor will offer actionable information to patients and their physicians.
Keywords: BRCA2; BRCAness; DNA repair; hereditary breast and ovarian cancer (HBOC); homologous recombination; variants of uncertain significance.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
BRCA2 BRC missense variants disrupt RAD51-dependent DNA repair.Elife. 2022 Sep 13;11:e79183. doi: 10.7554/eLife.79183. Elife. 2022. PMID: 36098506 Free PMC article.
-
Classification of BRCA2 Variants of Uncertain Significance (VUS) Using an ACMG/AMP Model Incorporating a Homology-Directed Repair (HDR) Functional Assay.Clin Cancer Res. 2022 Sep 1;28(17):3742-3751. doi: 10.1158/1078-0432.CCR-22-0203. Clin Cancer Res. 2022. PMID: 35736817 Free PMC article.
-
Functional analysis and clinical classification of 462 germline BRCA2 missense variants affecting the DNA binding domain.Am J Hum Genet. 2024 Mar 7;111(3):584-593. doi: 10.1016/j.ajhg.2024.02.002. Epub 2024 Feb 27. Am J Hum Genet. 2024. PMID: 38417439 Free PMC article.
-
BRCA1/2 variants of unknown significance in hereditary breast and ovarian cancer (HBOC) syndrome: Looking for the hidden meaning.Crit Rev Oncol Hematol. 2022 Apr;172:103626. doi: 10.1016/j.critrevonc.2022.103626. Epub 2022 Feb 10. Crit Rev Oncol Hematol. 2022. PMID: 35150867 Review.
-
Functional assays for analysis of variants of uncertain significance in BRCA2.Hum Mutat. 2014 Feb;35(2):151-64. doi: 10.1002/humu.22478. Epub 2013 Dec 3. Hum Mutat. 2014. PMID: 24323938 Free PMC article. Review.
Cited by
-
Germinal mutations among patients with breast cancer in Colombia: is BRCA3 coming?Ecancermedicalscience. 2025 Feb 27;19:1859. doi: 10.3332/ecancer.2025.1859. eCollection 2025. Ecancermedicalscience. 2025. PMID: 40259910 Free PMC article.
-
Inherited Mutations in DNA Damage Repair Genes in Italian Men with Metastatic Prostate Cancer: Results from the Meet-URO 10 Study.Eur Urol Open Sci. 2024 Feb 7;61:44-51. doi: 10.1016/j.euros.2024.01.015. eCollection 2024 Mar. Eur Urol Open Sci. 2024. PMID: 38384439 Free PMC article.
-
Reclassifying BRCA1 c.4358-2A > G and BRCA2 c.475 + 5G > C variants from "Uncertain Significance" to "Pathogenic" based on minigene assays and clinical evidence.J Cancer Res Clin Oncol. 2024 Feb 1;150(2):62. doi: 10.1007/s00432-023-05597-y. J Cancer Res Clin Oncol. 2024. PMID: 38300310 Free PMC article.
-
The Pathogenic R3052W BRCA2 Variant Disrupts Homology-Directed Repair by Failing to Localize to the Nucleus.Front Genet. 2022 May 30;13:884210. doi: 10.3389/fgene.2022.884210. eCollection 2022. Front Genet. 2022. PMID: 35711920 Free PMC article.
-
BRCA2 BRC missense variants disrupt RAD51-dependent DNA repair.Elife. 2022 Sep 13;11:e79183. doi: 10.7554/eLife.79183. Elife. 2022. PMID: 36098506 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
