

Three-Year Follow-Up of Laser In Situ Keratomileusis Treatments for Myopia: Multi-Center Cohort Study in Korean Population
- PMID: 34065718
- PMCID: PMC8156820
- DOI: 10.3390/jpm11050419
Three-Year Follow-Up of Laser In Situ Keratomileusis Treatments for Myopia: Multi-Center Cohort Study in Korean Population
Abstract
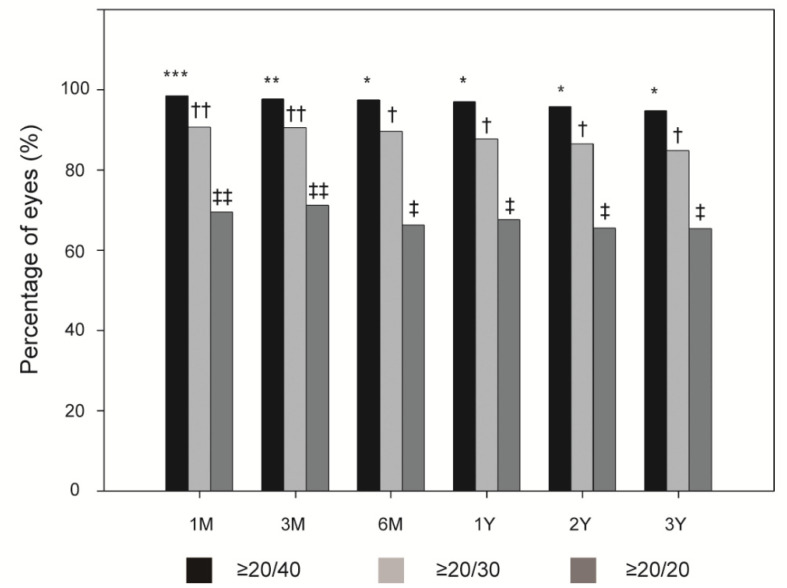
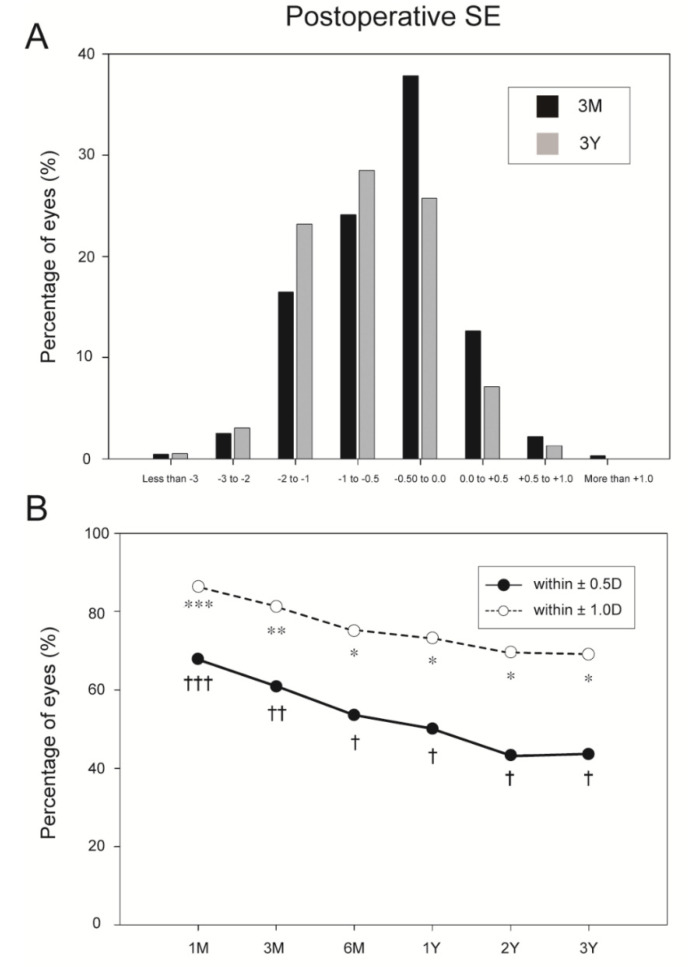
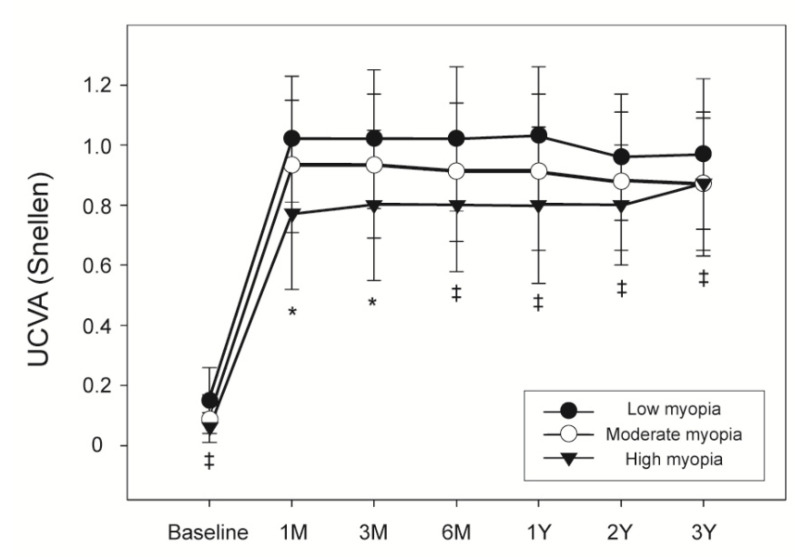
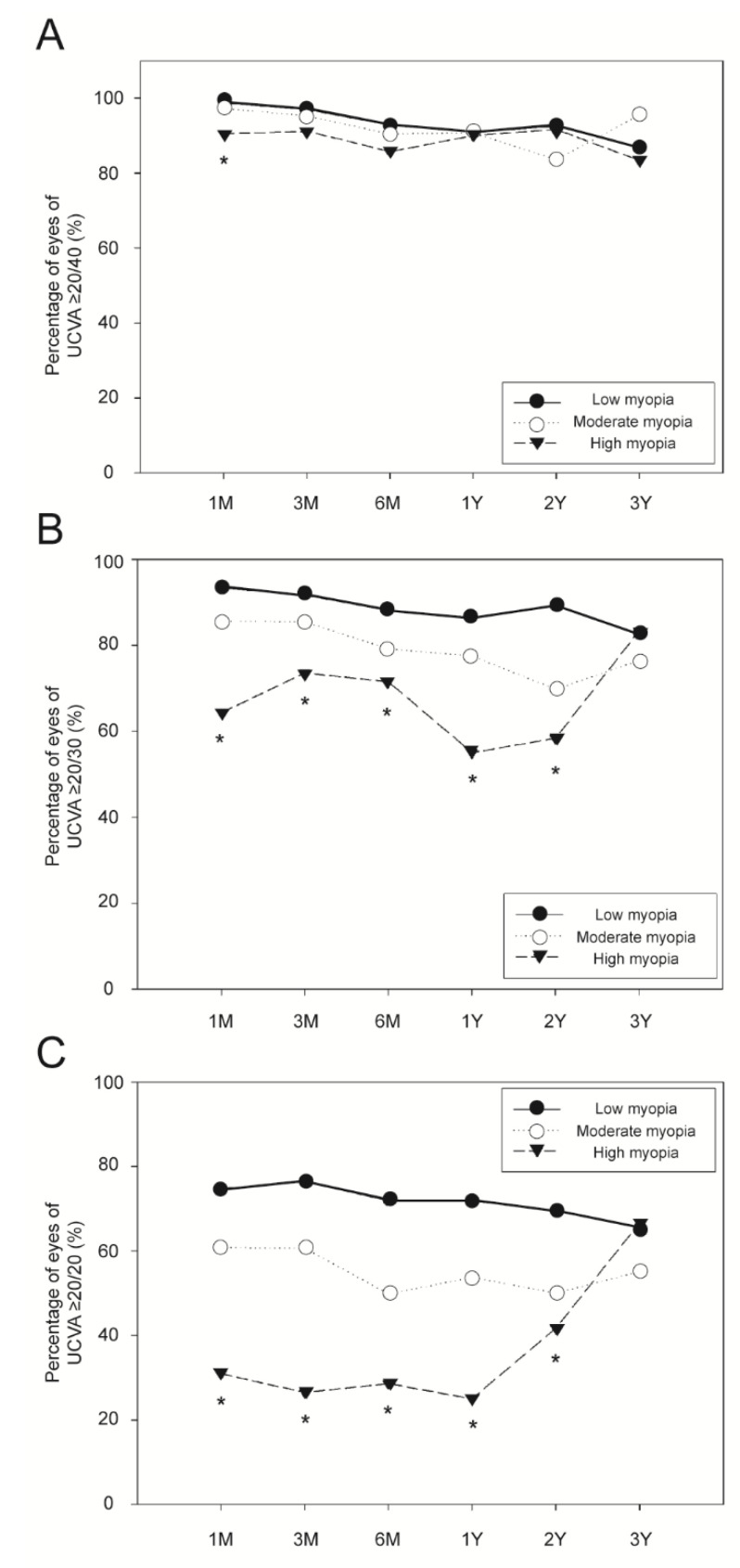
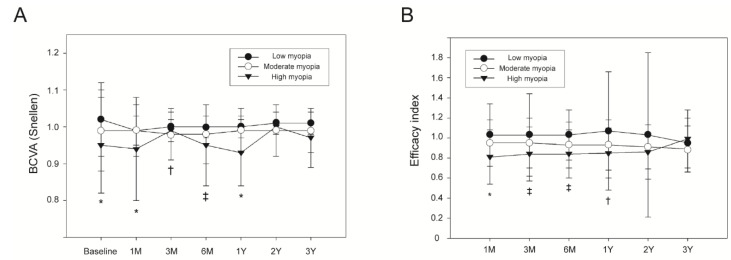
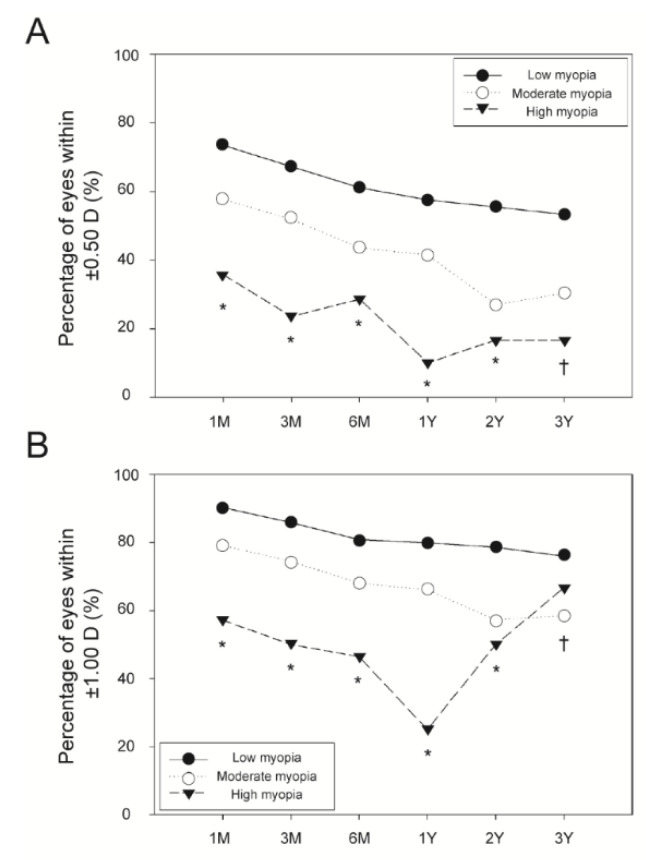
This multi-center cohort study included 3401 myopic laser in situ keratomileusis (LASIK) procedures conducted in 1756 myopia patients between 2002 and 2005. Pre- and postoperative uncorrected visual acuity (UCVA), best corrected visual acuity (BCVA), and manifest refraction spherical equivalent (SE) were recorded. Factors predicting low postoperative efficacy (defined as a postoperative UCVA < 0.5) were identified using univariate and multivariate logistic regression analysis. Compared with 1 month postoperatively, logMAR UCVA at 3 months postoperatively was significantly decreased (p = 0.002) and that at 2 and 3 years was significantly increased (p < 0.001). LogMAR BCVA at 2 years postoperatively was significantly decreased compared with 1 month postoperatively (p = 0.008). Over the 3-year postoperative period, overall refractive predictability within ±1.00 D and ±0.50 D ranged from 69.0% to 86.2% and from 43.3% to 67.8%, respectively. This also decreased from 1 month to 6 months postoperatively (p < 0.005). Multivariate logistic regression analysis using generalized estimating equations, revealed that higher preoperative SE (odds ratio [OR], 2.58 and 7.23; p < 0.001) and lower preoperative BCVA (OR, 2.44; p = 0.003) were predictive of a low postoperative efficacy. In summary, myopic LASIK can be effective and safe with a high refractive predictability in a Korean population, but myopic regression occurs over time. Higher preoperative SE and lower preoperative BCVA are predictive of a low postoperative efficacy.
Keywords: efficacy; laser in situ keratomileusis; safety.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
Spherical and aspherical photorefractive keratectomy and laser in-situ keratomileusis for moderate to high myopia: two prospective, randomized clinical trials. Summit technology PRK-LASIK study group.Trans Am Ophthalmol Soc. 1998;96:197-221; discussion 221-7. Trans Am Ophthalmol Soc. 1998. PMID: 10360290 Free PMC article. Clinical Trial.
-
[Laser in situ keratomyleusis (LASIK) for correction of myopia and hypermetropia--our one year experience].Vojnosanit Pregl. 2009 Dec;66(12):979-84. doi: 10.2298/vsp0912979v. Vojnosanit Pregl. 2009. PMID: 20095518 Serbian.
-
The effect of flap thickness on the visual and refractive outcome of myopic laser in situ keratomileusis.Eye (Lond). 2005 Dec;19(12):1290-6. doi: 10.1038/sj.eye.6701775. Eye (Lond). 2005. PMID: 15618975
-
Correction of myopia and myopic astigmatism by femtosecond laser in situ keratomileusis.Cesk Slov Oftalmol. 2019 Summer;75(2):65-71. doi: 10.31348/2019/2/2. Cesk Slov Oftalmol. 2019. PMID: 31537074 English.
-
Comparison of visual quality after Femto-LASIK and TransPRK in patients with low and moderate myopia.Int Ophthalmol. 2020 Jun;40(6):1419-1428. doi: 10.1007/s10792-020-01308-5. Epub 2020 Feb 19. Int Ophthalmol. 2020. PMID: 32076966
Cited by
-
Reversal of Myopic Correction for Patients Intolerant to LASIK.J Ophthalmol. 2021 Dec 15;2021:7113676. doi: 10.1155/2021/7113676. eCollection 2021. J Ophthalmol. 2021. PMID: 34956671 Free PMC article.
-
Long-Term Results of Laser In Situ Keratomileusis in Myopic Patients with Topographic Indices outside Suggested Ranges.Ophthalmol Ther. 2022 Dec;11(6):2285-2295. doi: 10.1007/s40123-022-00589-6. Epub 2022 Oct 12. Ophthalmol Ther. 2022. PMID: 36223055 Free PMC article.
References
-
- Kahuam-Lopez N., Navas A., Castillo-Salgado C., Graue-Hernandez E.O., Jimenez-Corona A., Ibarra A. Laser-assisted in-situ keratomileusis (lasik) with a mechanical microkeratome compared to lasik with a femtosecond laser for lasik in adults with myopia or myopic astigmatism. Cochrane Database Syst. Rev. 2020;4:CD012946. - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
