

A Practical Guide for the Management of Steroid Induced Hyperglycaemia in the Hospital
- PMID: 34065762
- PMCID: PMC8157052
- DOI: 10.3390/jcm10102154
A Practical Guide for the Management of Steroid Induced Hyperglycaemia in the Hospital
Abstract
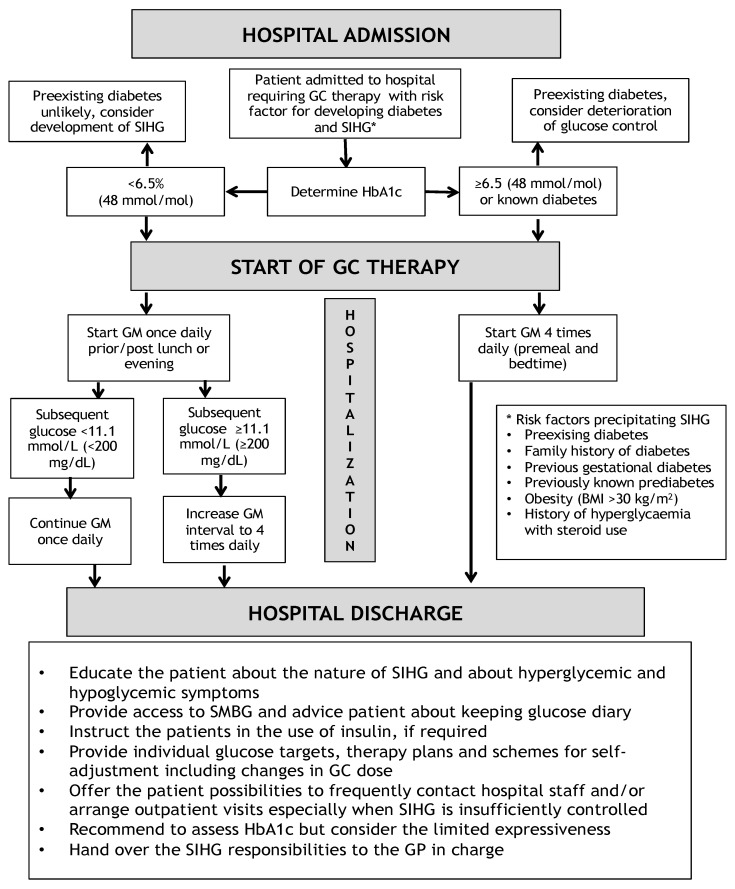
Glucocorticoids represent frequently recommended and often indispensable immunosuppressant and anti-inflammatory agents prescribed in various medical conditions. Despite their proven efficacy, glucocorticoids bear a wide variety of side effects among which steroid induced hyperglycaemia (SIHG) is among the most important ones. SIHG, potentially causes new-onset hyperglycaemia or exacerbation of glucose control in patients with previously known diabetes. Retrospective data showed that similar to general hyperglycaemia in diabetes, SIHG in the hospital and in outpatient settings detrimentally impacts patient outcomes, including mortality. However, recommendations for treatment targets and guidelines for in-hospital as well as outpatient therapeutic management are lacking, partially due to missing evidence from clinical studies. Still, SIHG caused by various types of glucocorticoids is a common challenge in daily routine and clinical guidance is needed. In this review, we aimed to summarize clinical evidence of SIHG in inpatient care impacting clinical outcome, establishment of diagnosis, diagnostic procedures and therapeutic recommendations.
Keywords: hospital; practical guide; steroid induced hyperglycaemia.
Conflict of interest statement
F.A. received speaker honoraria from Eli Lilly, Merck Sharp & Dome, Boehringer Ingelheim, Astra Zeneca and travel grants from Sanofi, Novo Nordisk, Takeda, Merck Sharp & Dome and Amgen. D.A.H. received travel grants from NovoNordisk, Novartis and Eli Lilly. H.S. received research grants from Boehringer Ingelheim, Eli Lilly, MSD, NovoNordisk and Sanofi. H.S. received lecture fees or honoraria for advisory boards from AstraZeneca, BMS, Boehringer Ingelheim, Eli Lilly, MSD, Novartis, NovoNordisk, Sanofi. J.K.M. is a member in the advisory board of Becton-Dickinson, Boehringer Ingelheim, Eli Lilly, Medtronic, Prediktor SA and Sanofi and received speaker honoraria from Abbott Diabetes Care, Astra Zeneca, Eli Lilly, Dexcom, Medtronic, Novo Nordisk, Roche Diabetes Care, Sanofi, Servier and Takeda.
Figures

References
-
- van Raalte D.H., Diamant M. Steroid diabetes: From mechanism to treatment? Neth. J. Med. 2014;72:62–72. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
