

Leriche Syndrome Misdiagnosed as Complex Regional Pain Syndrome in a Patient with Neuropathic Pain Caused by a Chip Fracture: A Case Report
- PMID: 34066172
- PMCID: PMC8150991
- DOI: 10.3390/medicina57050486
Leriche Syndrome Misdiagnosed as Complex Regional Pain Syndrome in a Patient with Neuropathic Pain Caused by a Chip Fracture: A Case Report
Abstract
Introduction: Leriche syndrome is an aortoiliac occlusive disease caused by atherosclerotic occlusion. We report a case of Leriche syndrome with a fracture that was suspected as complex regional pain syndrome (CRPS), as the post-traumatic pain gradually worsened in the form of excruciating neuropathic pain.
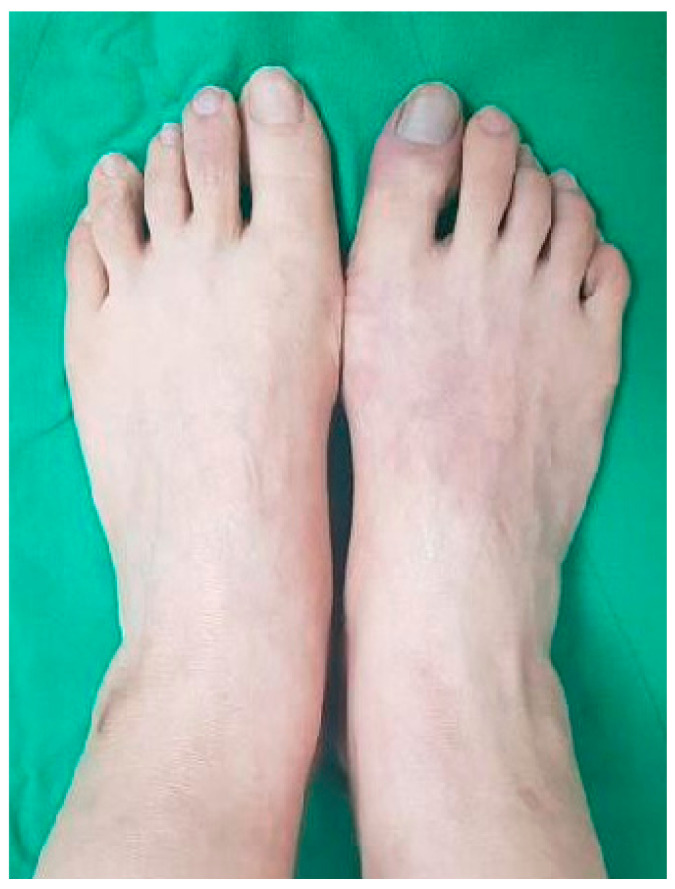
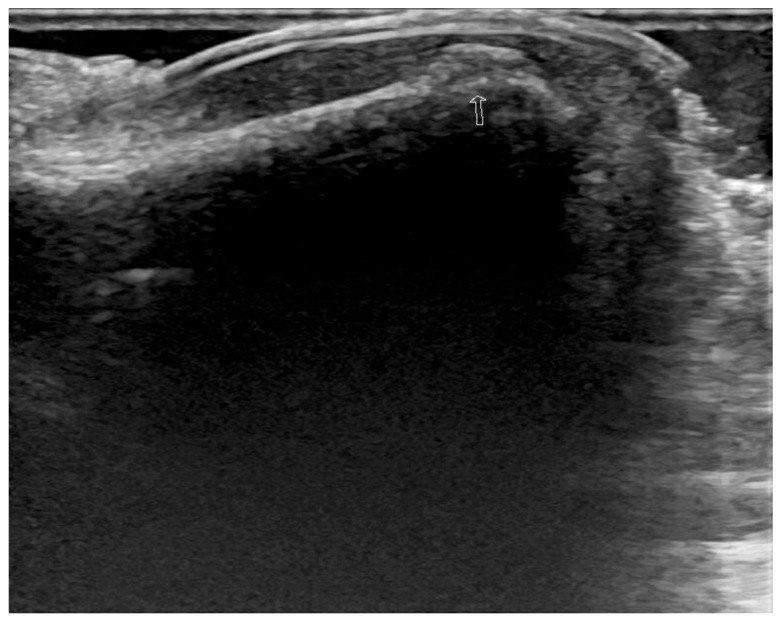
Case report: A 52-year-old woman with a history of hypertension was referred to the Department of Pain Medicine from a local orthopedic clinic because of suspected CRPS for excruciating neuropathic pain for one month. She complained of gait dysfunction and severe pain in the right foot following an incident of trauma with the right first toe. The average pain intensity assessed using the visual analog scale (VAS) was 90 (0: no pain, 100: the worst pain imaginable), and the neuropathic pain was evident as a score of 6/10 on Douleur neuropathique 4. Allodynia, hyperalgesia, blue discoloration of the skin, asymmetric temperature change (1.38 °C), and edematous soft tissue changes were observed. Ultrasonography showed a chip fracture in the first distal phalanx of the right first toe. The diagnosis was most probably CRPS type I according to the Budapest research criteria for CRPS. However, multiple pain management techniques were insufficient in controlling the symptoms. A month and a half later, an ankle-brachial index score of less than 0.4 suggested severe peripheral artery disease. Computed tomography angiography showed total occlusion between the infrarenal abdominal aorta and the bilateral common iliac arteries. Therefore, she underwent aortic-bifemoral bypass surgery with a diagnosis of Leriche syndrome. Three months after the surgery, the average pain intensity was graded as 10 on the VAS (0-100), the color of the skin of the right first toe improved and no gait dysfunction was observed.
Conclusion: A chip fracture in a region with insufficient blood flow could manifest as excruciating neuropathic pain in Leriche syndrome.
Keywords: Leriche syndrome; claudication; complex regional pain syndrome; neuropathic pain; peripheral arterial disease.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
[Leriche syndrome].Agri. 2017 Jan;29(1):38-42. doi: 10.5505/agri.2015.65983. Agri. 2017. PMID: 28467568 Turkish.
-
[Surgery of abdominal aorta with horseshoe kidney].Srp Arh Celok Lek. 1997 Jan-Feb;125(1-2):36-44. Srp Arh Celok Lek. 1997. PMID: 17974353 Serbian.
-
Right calf claudication revealing leriche syndrome presenting as right sciatic neuropathy.Ann Rehabil Med. 2014 Feb;38(1):132-7. doi: 10.5535/arm.2014.38.1.132. Epub 2014 Feb 25. Ann Rehabil Med. 2014. PMID: 24639938 Free PMC article.
-
Anatomical significance in aortoiliac occlusive disease.Clin Anat. 2014 Nov;27(8):1264-74. doi: 10.1002/ca.22444. Epub 2014 Jul 25. Clin Anat. 2014. PMID: 25065617 Review.
-
Leriche syndrome in a patient with acute pulmonary embolism and acute myocardial infarction: a case report and review of literature.BMC Cardiovasc Disord. 2020 Jan 17;20(1):26. doi: 10.1186/s12872-019-01288-0. BMC Cardiovasc Disord. 2020. PMID: 31952498 Free PMC article. Review.
Cited by
-
Aortoiliac Occlusion in a Rare Instance of Leriche Syndrome Type I in a 65-Year-Old Woman With Chronic Leg Discomfort Refractory to Pregabalin.Cureus. 2023 Nov 15;15(11):e48858. doi: 10.7759/cureus.48858. eCollection 2023 Nov. Cureus. 2023. PMID: 38106757 Free PMC article.
-
Antiphospholipid Syndrome-Induced Leriche Syndrome in a Man with Lower Limbs Sensory and Motor Defect.J Cardiovasc Dev Dis. 2021 Aug 29;8(9):104. doi: 10.3390/jcdd8090104. J Cardiovasc Dev Dis. 2021. PMID: 34564122 Free PMC article.
-
Leriche syndrome diagnosed due to polytrauma: a case report.Int J Emerg Med. 2022 Feb 4;15(1):8. doi: 10.1186/s12245-022-00411-x. Int J Emerg Med. 2022. PMID: 35120433 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
