

Ichthyoses-A Clinical and Pathological Spectrum from Heterogeneous Cornification Disorders to Inflammation
- PMID: 34066992
- PMCID: PMC8161842
- DOI: 10.3390/dermatopathology8020017
Ichthyoses-A Clinical and Pathological Spectrum from Heterogeneous Cornification Disorders to Inflammation
Abstract
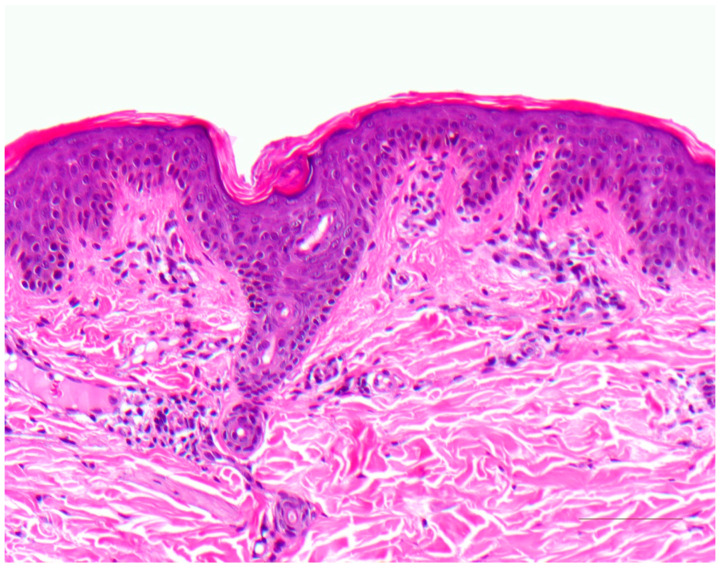
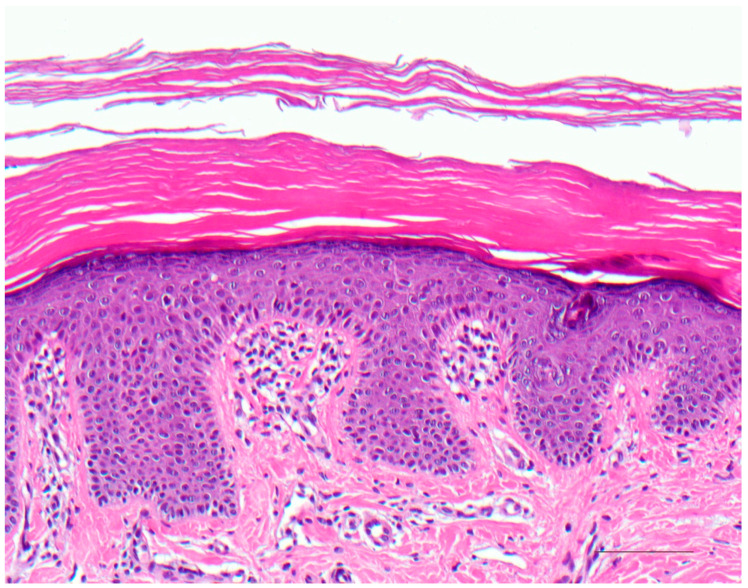
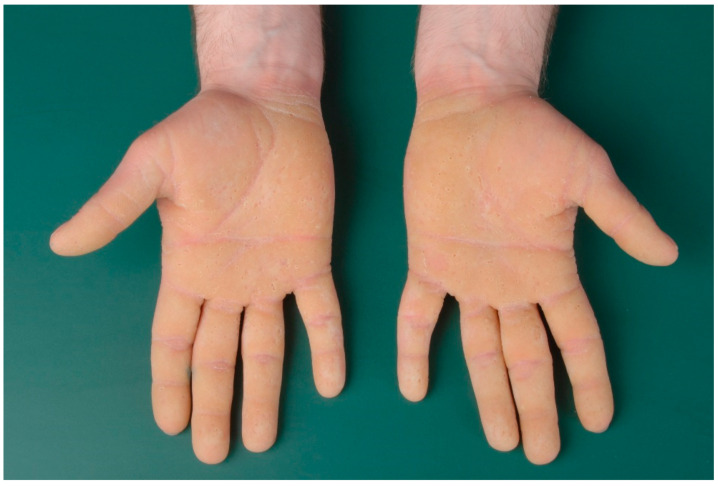
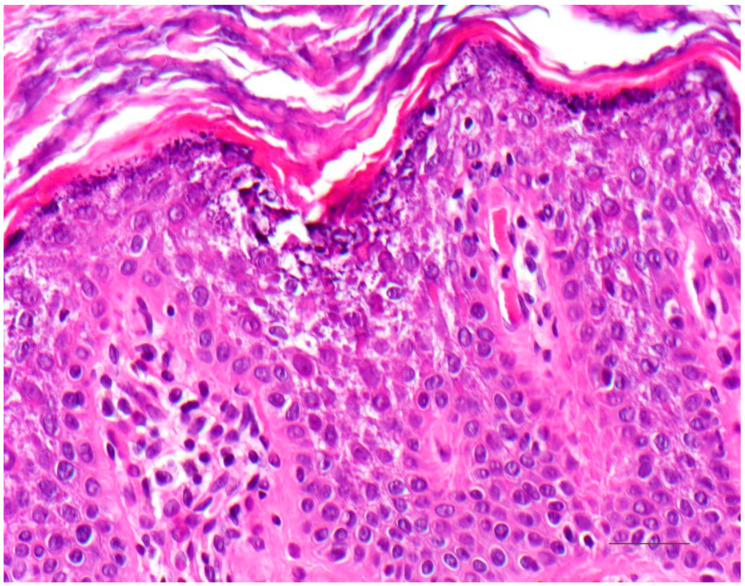
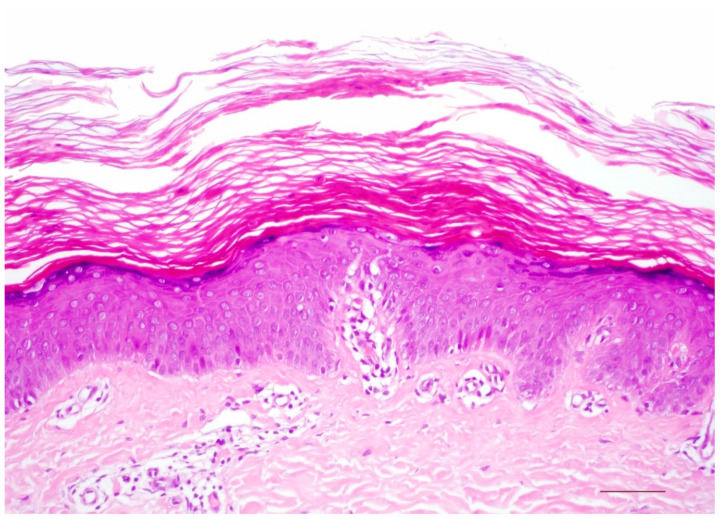
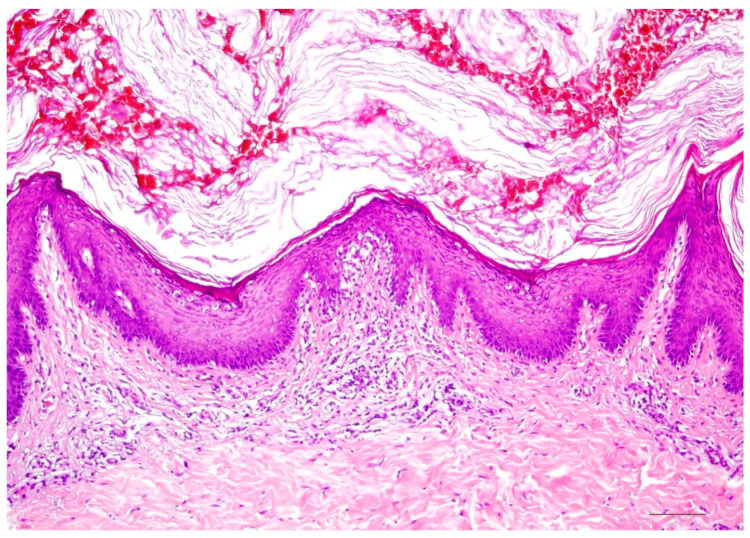
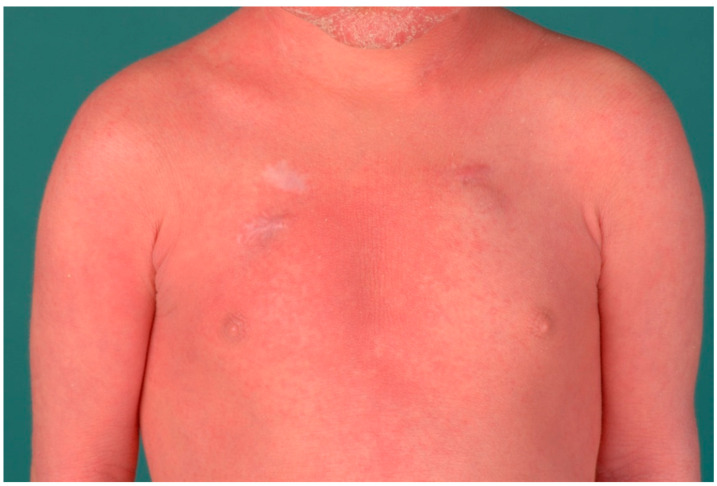
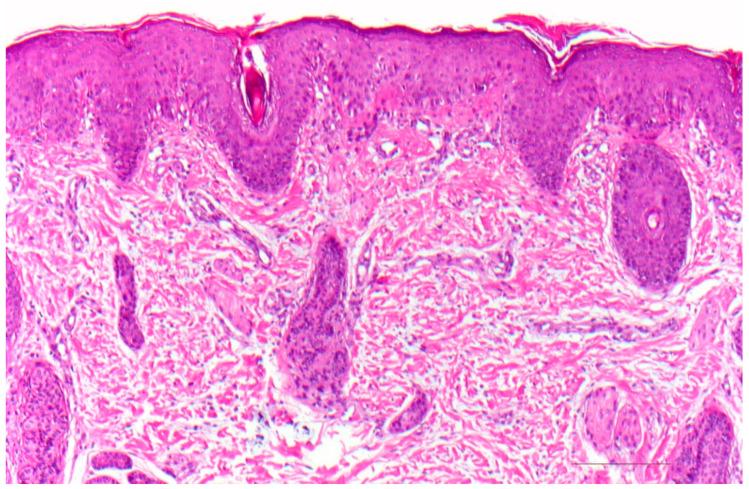
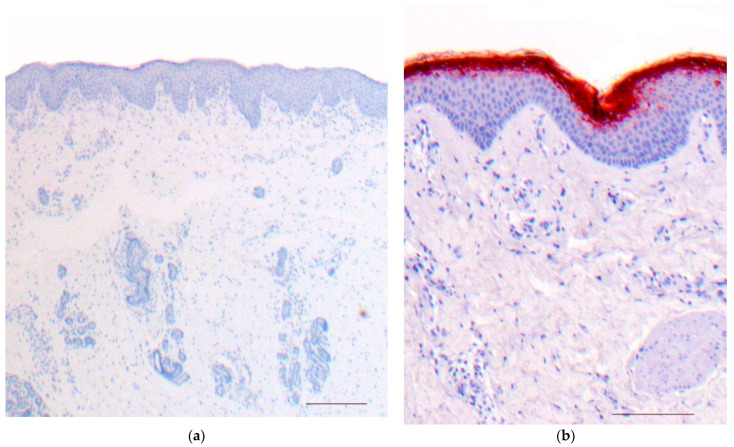
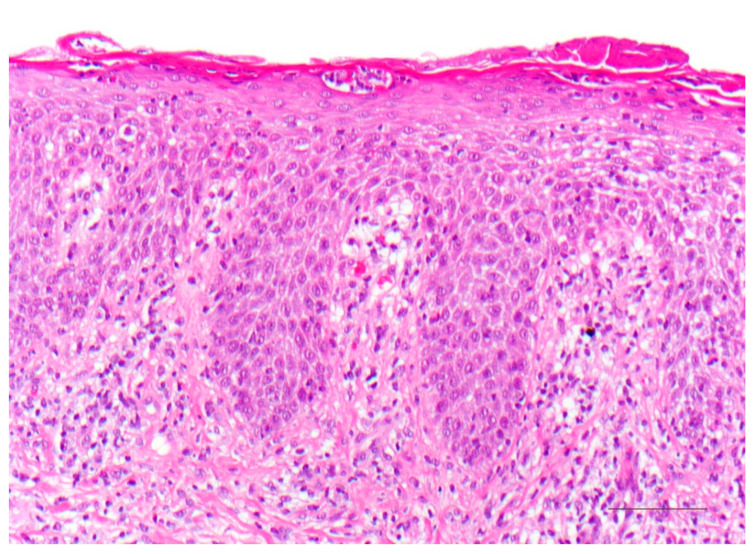
Ichthyoses are inborn keratinization disorders affecting the skin only (non-syndromic) or are associated with diseases of internal organs (syndromic). In newborns, they can be life-threatening. The identification of the gene defects resulted in reclassification and a better understanding of the pathophysiology. Histopathologic patterns include orthohyperkeratosis with a reduced or well-developed stratum granulosum, hyperkeratosis with ortho- and parakeratosis with preserved or prominent stratum granulosum, and epidermolytic ichthyosis. Another pattern features "perinuclear vacuoles and binucleated keratinocytes", which is associated with keratin mutations. Some ichthyoses are histologically defined by psoriasis-like features, and distinct subtypes show follicular hyperkeratosis. In addition to histological and immunohistochemical methods, these patterns allow a better histopathologic diagnosis.
Keywords: dermatopathology; hereditary keratinization disorders; ichthyosis; immunohistochemistry; pattern analysis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Traupe H. A Guide to Clinical Diagnosis, Genetic Counseling, and Therapy. Springer; Berlin, Germany: 1989. The Ichthyoses; pp. 103–138.
-
- Oji V., Traupe H. Ichthyoses: Differential diagnosis and molecular genetics. Eur. J. Dermatol. 2006;16:349–359. - PubMed
-
- Oji V., Tadini G., Akiyama M., Blanchet Bardon C., Bodemer C., Bourrat E., Coudiere P., DiGiovanna J.J., Elias P., Fischer J., et al. Revised nomenclature and classification of inherited ichthyoses: Results of the First Ichthyosis Consensus Conference in Sorèze 2009. J. Am. Acad. Dermatol. 2010;63:607–641. doi: 10.1016/j.jaad.2009.11.020. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
