

Radial Access for Coronary Angiography Carries Fewer Complications Compared with Femoral Access: A Meta-Analysis of Randomized Controlled Trials
- PMID: 34067672
- PMCID: PMC8156941
- DOI: 10.3390/jcm10102163
Radial Access for Coronary Angiography Carries Fewer Complications Compared with Femoral Access: A Meta-Analysis of Randomized Controlled Trials
Abstract
Background and aim: In patients undergoing diagnostic coronary angiography (CA) and percutaneous coronary interventions (PCI), the benefits associated with radial access compared with the femoral access approach remain controversial. The aim of this meta-analysis was to compare the short-term evidence-based clinical outcome of the two approaches.
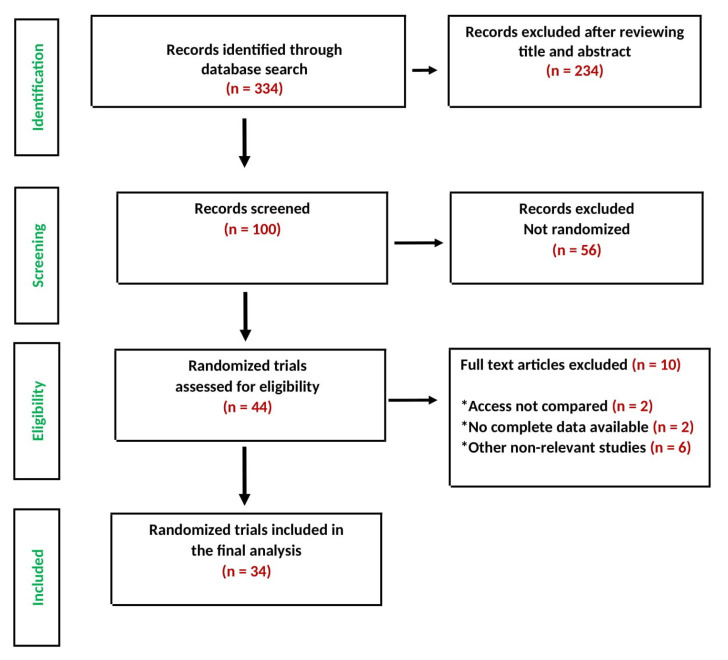
Methods: The PubMed, Embase, Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov databases were searched for randomized controlled trials (RCTs) comparing radial versus femoral access for CA and PCI. We identified 34 RCTs with 29,352 patients who underwent CA and/or PCI and compared 14,819 patients randomized for radial access with 14,533 who underwent procedures using femoral access. The follow-up period for clinical outcome was 30 days in all studies. Data were pooled by meta-analysis using a fixed-effect or a random-effect model, as appropriate. Risk ratios (RRs) were used for efficacy and safety outcomes.
Results: Compared with femoral access, the radial access was associated with significantly lower risk for all-cause mortality (RR: 0.74; 95% confidence interval (CI): 0.61 to 0.88; p = 0.001), major bleeding (RR: 0.53; 95% CI:0.43 to 0.65; p ˂ 0.00001), major adverse cardiovascular events (MACE)(RR: 0.82; 95% CI: 0.74 to 0.91; p = 0.0002), and major vascular complications (RR: 0.37; 95% CI: 0.29 to 0.48; p ˂ 0.00001). These results were consistent irrespective of the clinical presentation of ACS or STEMI.
Conclusions: Radial access in patients undergoing CA with or without PCI is associated with lower mortality, MACE, major bleeding and vascular complications, irrespective of clinical presentation, ACS or STEMI, compared with femoral access.
Keywords: PCI; acute coronary syndrome; coronarography; femoral; radial; stable coronary artery disease.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Habib R.H., Dimitrova K.R., Badour S.A., Yammine M.B., El-Hage-Sleiman A.K.M., Hoffman D.M., Geller C.M., Schwann T.A., Tranbaugh R.F. CABG Versus PCI: Greater Benefit in Long-Term Outcomes with Multiple Arterial Bypass Grafting. J. Am. Coll. Cardiol. 2015;66:1417–1427. doi: 10.1016/j.jacc.2015.07.060. - DOI - PMC - PubMed
-
- Venkitachalam L., Kip K.E., Selzer F., Wilensky R.L., Slater J., Mulukutla S.R., Marroquin O.C., Block P.C., Williams D.O., Kelsey S.F. Twenty-year evolution of percutaneous coronary intervention and its impact on clinical outcomes: A report from the National Heart, Lung, and Blood Institute-sponsored, multicenter 1985–1986 PTCA and 1997–2006 dynamic registries. Circ. Cardiovasc. Interv. 2009;2:6–13. doi: 10.1161/CIRCINTERVENTIONS.108.825323. - DOI - PMC - PubMed
-
- Rao S.V., O’Grady K., Pieper K.S., Granger C.B., Newby L.K., Van de Werf F., Mahaffey K.W., Califf R.M., Harrington R.A. Impact of Bleeding Severity on Clinical Outcomes Among Patients With Acute Coronary Syndromes. Am. J. Cardiol. 2005;96:1200–1206. doi: 10.1016/j.amjcard.2005.06.056. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
