

Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York
- PMID: 34067743
- PMCID: PMC8156250
- DOI: 10.3390/vaccines9050516
Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York
Abstract
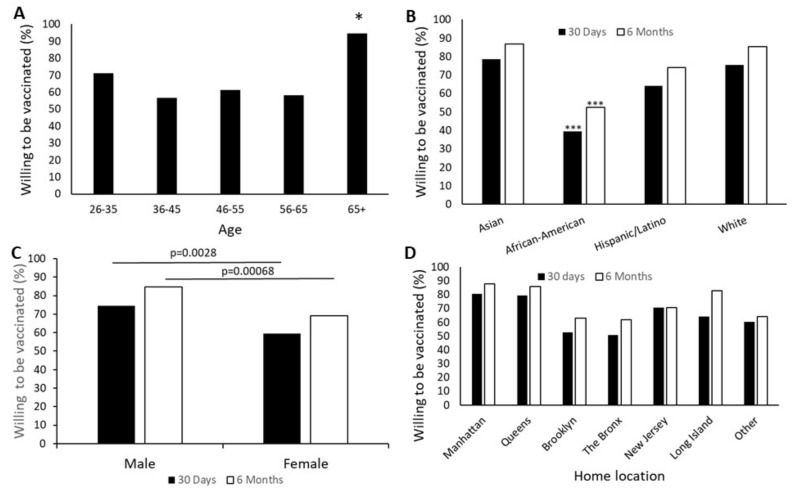
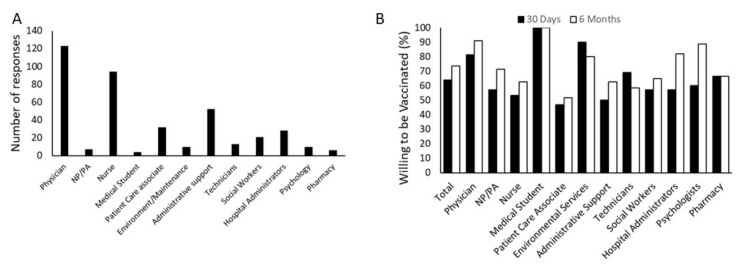
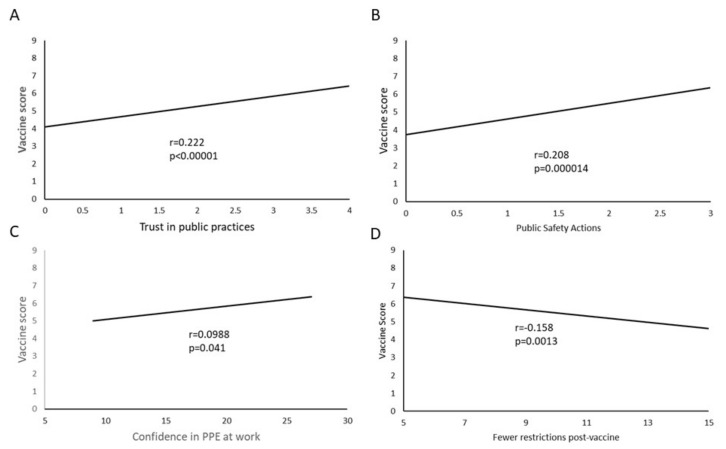
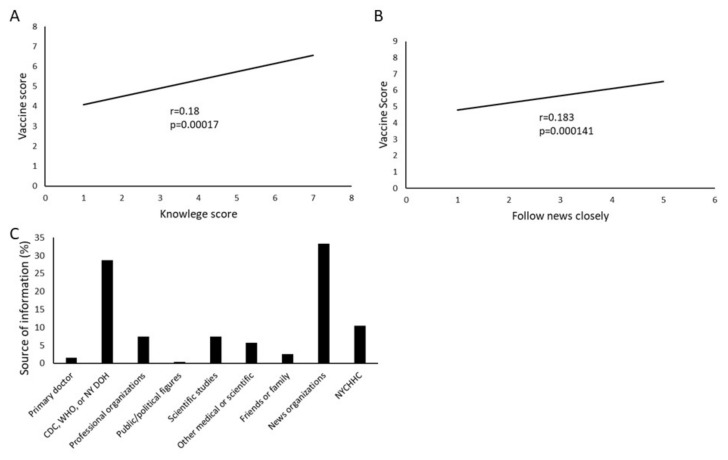
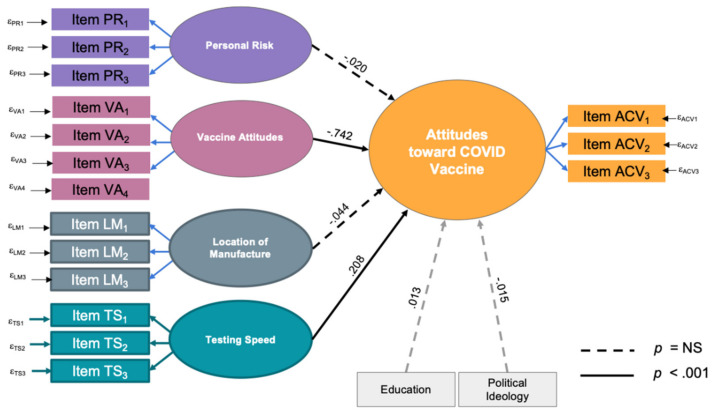
Introduction: New York City is one of the areas most affected by the COVID-19 pandemic in the United States. Healthcare workers are among those at high risk of contracting the virus, and a vital source of information and trust in vaccines to the community. Methods: This study was conducted about attitudes towards COVID-19 vaccination among healthcare workers at a public hospital in New York City during the beginning of COVID-19 vaccination. 428 hospital employees responded. Results: Several factors were significantly associated with vaccine attitudes, including demographics such as gender (p = 0.002), age (p = 0.005), race (p < 0.001) and home location (p < 0.001), role within the hospital (p < 0.001), knowledge about the virus (p < 0.001) and confidence in and expectations about personal protective equipment and behaviors (p < 0.001). Structural equation modeling revealed that the most predictive factors were prior vaccine attitudes and concern with the speed of testing and approval of the vaccines (p < 0.001). Multivariate analysis reinforced these, while also identifying perceived personal risk as significant (p = 0.033). Conclusions: Several modifiable factors that reflect confidence in science, scientific knowledge, personal risk perception, experience and medical authority are correlated with vaccine attitudes, indicating that a holistic educational approach to improve trust in science is likely to be effective in long-term reduction in vaccine hesitancy.
Keywords: COVID-19; healthcare workers; vaccine attitudes; vaccine hesitancy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. [(accessed on 27 February 2021)]; Available online: https://coronavirus.jhu.edu/map.html.
-
- WHO Draft Landscape and Tracker of COVID-19 Candidate Vaccines. [(accessed on 27 February 2021)]; Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-cand....
-
- Ten Threats to Global Health in 2019. [(accessed on 3 March 2021)]; Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-....
-
- Funk C., Tyson A. Intent to Get a COVID-19 Vaccine Rises to 60% as Confidence in Research and Development Process Increases. Pew Research Center. [(accessed on 16 May 2021)];2020 Dec 3; Available online: https://www.pewresearch.org/science/2020/12/03/intent-to-get-a-covid-19-...
LinkOut - more resources
Full Text Sources
