

An Interaction Effect Analysis of Thermodilution-Guided Hemodynamic Optimization, Patient Condition, and Mortality after Successful Cardiopulmonary Resuscitation
- PMID: 34068997
- PMCID: PMC8156244
- DOI: 10.3390/ijerph18105223
An Interaction Effect Analysis of Thermodilution-Guided Hemodynamic Optimization, Patient Condition, and Mortality after Successful Cardiopulmonary Resuscitation
Abstract
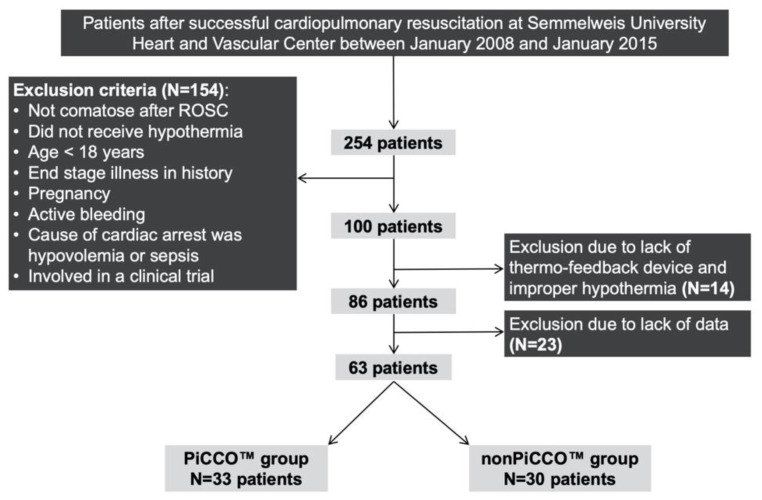
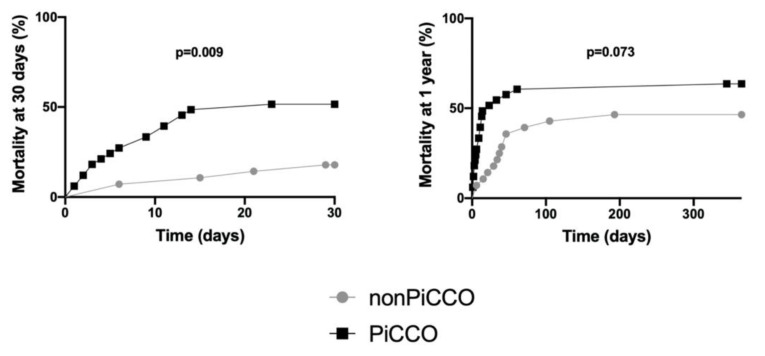
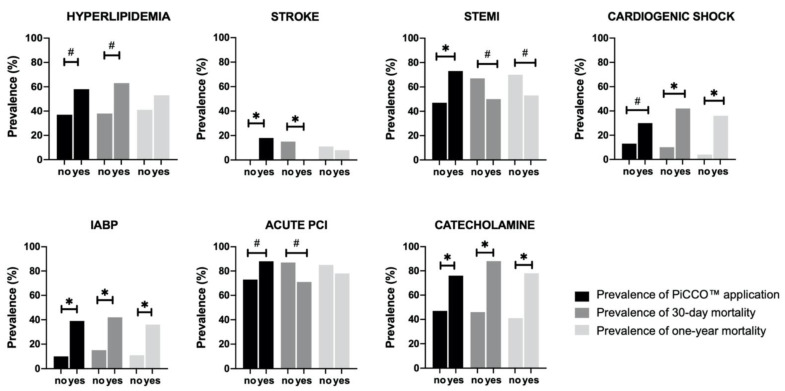
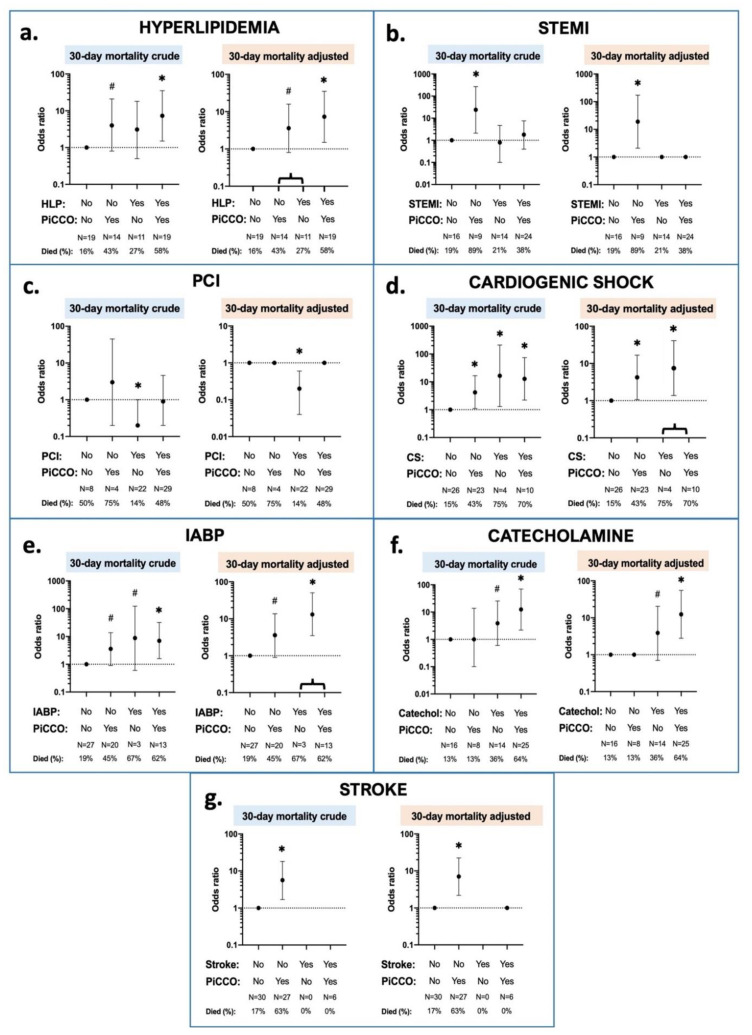
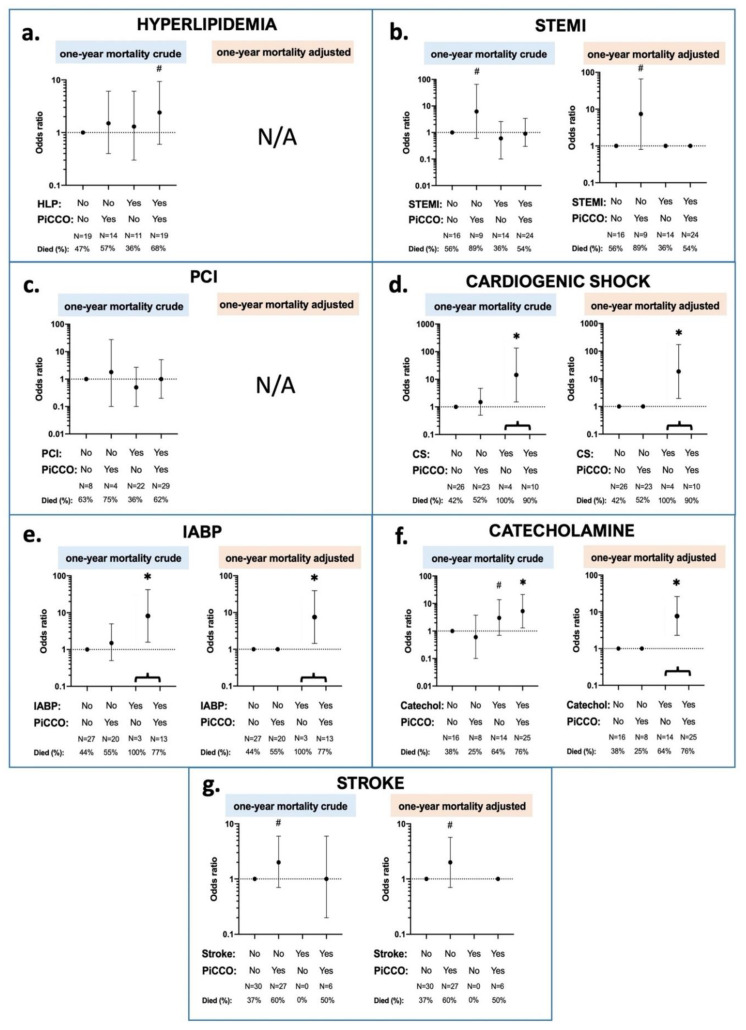
Proper hemodynamic management is necessary among post-cardiac arrest patients to improve survival. We aimed to investigate the effects of PiCCO™-guided (pulse index contour cardiac output) hemodynamic management on mortality in post-resuscitation therapy. In this longitudinal analysis of 63 comatose patients after successful cardiopulmonary resuscitation cooled to 32-34 °C, 33 patients received PiCCO™, and 30 were not monitored with PiCCO™. Primary and secondary outcomes were 30 day and 1 year mortality. Kaplan-Meier curves and log-rank tests were used to assess differences in mortality among the groups. Interaction effects to disentangle the relationship between patient's condition, PiCCO™ application, and mortality were assessed by means of Chi-square tests and logistic regression models. A 30 day mortality was significantly higher among PiCCO™ patients, while 1 year mortality was marginally higher. More severe patient condition per se was not the cause of higher mortality rate in the PiCCO™ group. Patients in better health conditions (without ST-elevation myocardial infarction, without cardiogenic shock, without intra-aortic balloon pump device, or without stroke in prior history) had worse outcomes with PiCCO™-guided therapy. Catecholamine administration worsened both 30 day and 1 year mortality among all patients. Our analysis showed that there was a complex interaction relationship between PiCCO™-guided therapy, patients' condition, and 30 day mortality for most conditions.
Keywords: cardiac arrest; hemodynamic monitoring; hypothermia; mortality; resuscitation; thermodilution.
Conflict of interest statement
The authors declare that they have no competing interest.
Figures
Similar articles
-
Impedance cardiography for aortic balloon counterpulsation impact assessment on patients hemodynamics during acute myocardial infarction.Medicina (Kaunas). 2006;42(11):904-13. Medicina (Kaunas). 2006. PMID: 17172792
-
Reliability of cardiac output measurements using LiDCOrapid™ and FloTrac/Vigileo™ across broad ranges of cardiac output values.J Clin Monit Comput. 2017 Aug;31(4):709-716. doi: 10.1007/s10877-016-9896-7. Epub 2016 Jun 14. J Clin Monit Comput. 2017. PMID: 27300325 Free PMC article.
-
Accuracy and precision of transcardiopulmonary thermodilution in patients with cardiogenic shock.J Clin Monit Comput. 2016 Dec;30(6):849-856. doi: 10.1007/s10877-015-9782-8. Epub 2015 Oct 1. J Clin Monit Comput. 2016. PMID: 26429134
-
Hemodynamic monitoring by transpulmonary thermodilution and pulse contour analysis in critically ill children.Pediatr Crit Care Med. 2011 Jul;12(4):459-66. doi: 10.1097/PCC.0b013e3182070959. Pediatr Crit Care Med. 2011. PMID: 21263372 Review.
-
Global end-diastolic volume an emerging preload marker vis-a-vis other markers - Have we reached our goal?Ann Card Anaesth. 2016 Oct-Dec;19(4):699-704. doi: 10.4103/0971-9784.191554. Ann Card Anaesth. 2016. PMID: 27716702 Free PMC article. Review.
Cited by
-
Cardiac arrest related lung edema: examining the role of downtimes in transpulmonary thermodilution analysis.Intern Emerg Med. 2024 Mar;19(2):501-509. doi: 10.1007/s11739-023-03420-7. Epub 2023 Sep 12. Intern Emerg Med. 2024. PMID: 37700181
-
[Cardiac resuscitation-associated lung edema (CRALE): evaluation of diagnostic and therapeutic approaches by an expert group of the German Cardiac Society].Med Klin Intensivmed Notfmed. 2025 Mar 24. doi: 10.1007/s00063-025-01268-7. Online ahead of print. Med Klin Intensivmed Notfmed. 2025. PMID: 40126642 German.
References
-
- Grasner J.T., Wnent J., Herlitz J., Perkins G.D., Lefering R., Tjelmeland I., Koster R.W., Masterson S., Rossell-Ortiz F., Maurer H., et al. Survival after out-of-hospital cardiac arrest in Europe—Results of the EuReCa TWO study. Resuscitation. 2020;148:218–226. doi: 10.1016/j.resuscitation.2019.12.042. - DOI - PubMed
-
- Kiguchi T., Okubo M., Nishiyama C., Maconochie I., Ong M.E.H., Kern K.B., Wyckoff M.H., McNally B., Christensen E.F., Tjelmeland I., et al. Out-of-hospital cardiac arrest across the World: First report from the International Liaison Committee on Resuscitation (ILCOR) Resuscitation. 2020;152:39–49. doi: 10.1016/j.resuscitation.2020.02.044. - DOI - PubMed
-
- Perkins G.D., Handley A.J., Koster R.W., Castren M., Smyth M.A., Olasveengen T., Monsieurs K.G., Raffay V., Grasner J.T., Wenzel V., et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 2. Adult basic life support and automated external defibrillation. Resuscitation. 2015;95:81–99. doi: 10.1016/j.resuscitation.2015.07.015. - DOI - PubMed
-
- Nolan J.P., Neumar R.W., Adrie C., Aibiki M., Berg R.A., Bottiger B.W., Callaway C., Clark R.S., Geocadin R.G., Jauch E.C., et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation. 2008;79:350–379. doi: 10.1016/j.resuscitation.2008.09.017. - DOI - PubMed
-
- Nolan J.P., Soar J., Cariou A., Cronberg T., Moulaert V.R., Deakin C.D., Bottiger B.W., Friberg H., Sunde K., Sandroni C. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines for Post-resuscitation Care 2015: Section 5 of the European Resuscitation Council Guidelines for Resuscitation 2015. Resuscitation. 2015;95:202–222. doi: 10.1016/j.resuscitation.2015.07.018. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
