

Utility of Different Surrogate Enzyme-Linked Immunosorbent Assays (sELISAs) for Detection of SARS-CoV-2 Neutralizing Antibodies
- PMID: 34069088
- PMCID: PMC8157164
- DOI: 10.3390/jcm10102128
Utility of Different Surrogate Enzyme-Linked Immunosorbent Assays (sELISAs) for Detection of SARS-CoV-2 Neutralizing Antibodies
Abstract
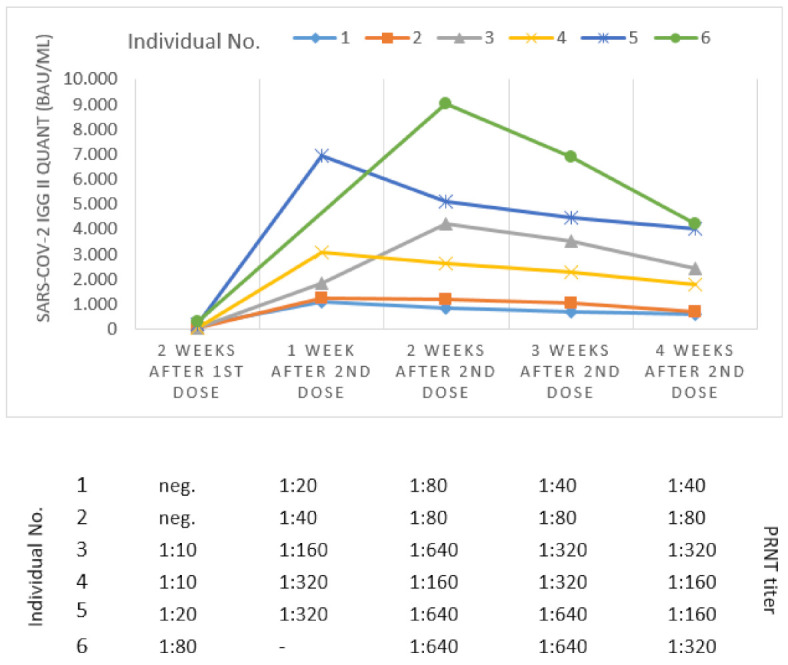
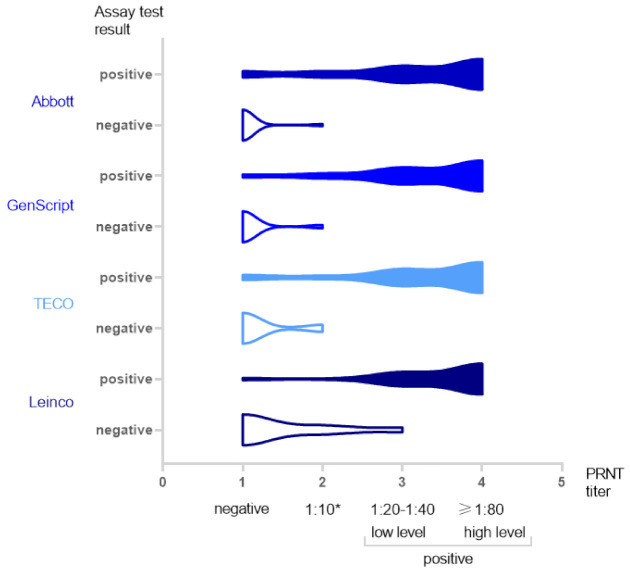
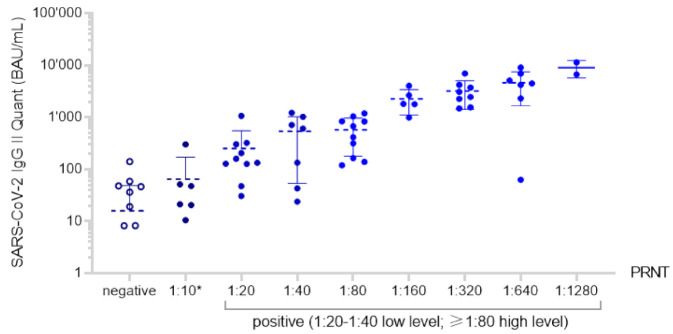
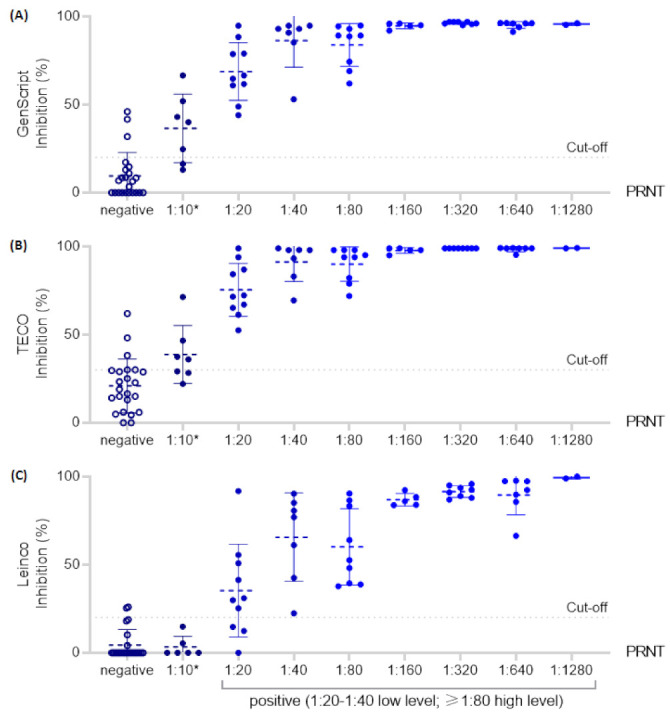
The plaque reduction neutralization test (PRNT) is a preferred method for the detection of functional, SARS-CoV-2 specific neutralizing antibodies from serum samples. Alternatively, surrogate enzyme-linked immunosorbent assays (ELISAs) using ACE2 as the target structure for the detection of neutralization-competent antibodies have been developed. They are capable of high throughput, have a short turnaround time, and can be performed under standard laboratory safety conditions. However, there are very limited data on their clinical performance and how they compare to the PRNT. We evaluated three surrogate immunoassays (GenScript SARS-CoV-2 Surrogate Virus Neutralization Test Kit (GenScript Biotech, Piscataway Township, NJ, USA), the TECO® SARS-CoV-2 Neutralization Antibody Assay (TECOmedical AG, Sissach, Switzerland), and the Leinco COVID-19 ImmunoRank™ Neutralization MICRO-ELISA (Leinco Technologies, Fenton, MO, USA)) and one automated quantitative SARS-CoV-2 Spike protein-based IgG antibody assay (Abbott GmbH, Wiesbaden, Germany) by testing 78 clinical samples, including several follow-up samples of six BNT162b2 (BioNTech/Pfizer, Mainz, Germany/New York, NY, USA) vaccinated individuals. Using the PRNT as a reference method, the overall sensitivity of the examined assays ranged from 93.8 to 100% and specificity ranged from 73.9 to 91.3%. Weighted kappa demonstrated a substantial to almost perfect agreement. The findings of our study allow these assays to be considered when a PRNT is not available. However, the latter still should be the preferred choice. For optimal clinical performance, the cut-off value of the TECO assay should be individually adapted.
Keywords: PRNT; SARS-CoV-2; neutralizing antibodies; surrogate ELISA.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Evaluating Humoral Immunity against SARS-CoV-2: Validation of a Plaque-Reduction Neutralization Test and a Multilaboratory Comparison of Conventional and Surrogate Neutralization Assays.Microbiol Spectr. 2021 Dec 22;9(3):e0088621. doi: 10.1128/Spectrum.00886-21. Epub 2021 Nov 17. Microbiol Spectr. 2021. PMID: 34787495 Free PMC article.
-
Two novel SARS-CoV-2 surrogate virus neutralization assays are suitable for assessing successful immunization with mRNA-1273.J Virol Methods. 2022 Jan;299:114297. doi: 10.1016/j.jviromet.2021.114297. Epub 2021 Sep 23. J Virol Methods. 2022. PMID: 34563583 Free PMC article.
-
Serological Assays for Assessing Postvaccination SARS-CoV-2 Antibody Response.Microbiol Spectr. 2021 Oct 31;9(2):e0073321. doi: 10.1128/Spectrum.00733-21. Epub 2021 Sep 29. Microbiol Spectr. 2021. PMID: 34585943 Free PMC article.
-
Evaluation of a commercial ELISA as alternative to plaque reduction neutralization test to detect neutralizing antibodies against SARS-CoV-2.Sci Rep. 2022 Mar 3;12(1):3549. doi: 10.1038/s41598-022-07597-3. Sci Rep. 2022. PMID: 35241780 Free PMC article.
-
Advances in Surrogate Neutralization Tests for High-Throughput Screening and the Point-of-Care.Anal Chem. 2025 Mar 18;97(10):5407-5423. doi: 10.1021/acs.analchem.5c00666. Epub 2025 Mar 4. Anal Chem. 2025. PMID: 40035475 Free PMC article. Review. No abstract available.
Cited by
-
Long-term decay of anti-RBD IgG titers after BNT162b2 vaccination is not mirrored by loss of neutralizing bioactivity against SARS-CoV-2.Clin Chim Acta. 2022 Jan 1;524:11-17. doi: 10.1016/j.cca.2021.11.023. Epub 2021 Nov 27. Clin Chim Acta. 2022. PMID: 34843705 Free PMC article.
-
Novel Competitive ELISA Utilizing Trimeric Spike Protein of SARS-CoV-2, Could Identify More Than RBD-RBM Specific Neutralizing Antibodies in Hybrid Sera.Vaccines (Basel). 2024 Aug 13;12(8):914. doi: 10.3390/vaccines12080914. Vaccines (Basel). 2024. PMID: 39204038 Free PMC article.
-
Boosting of the SARS-CoV-2-Specific Immune Response after Vaccination with Single-Dose Sputnik Light Vaccine.J Immunol. 2022 Mar 1;208(5):1139-1145. doi: 10.4049/jimmunol.2101052. Epub 2022 Jan 31. J Immunol. 2022. PMID: 35101893 Free PMC article.
-
Severe impairment of T-cell responses to BNT162b2 immunization in patients with multiple myeloma.Blood. 2022 Jan 6;139(1):137-142. doi: 10.1182/blood.2021013429. Blood. 2022. PMID: 34657156 Free PMC article. No abstract available.
-
Severe Acute Respiratory Syndrome Coronavirus 2 Antibody Response After Heterologous Immunizations With ChAdOx1/BNT162b2 in End-Stage Renal Disease Patients on Hemodialysis.Front Immunol. 2022 Jun 6;13:894700. doi: 10.3389/fimmu.2022.894700. eCollection 2022. Front Immunol. 2022. PMID: 35734170 Free PMC article.
References
-
- WHO World Health Organization Coronavirus Disease (COVID-19) Dashboard. [(accessed on 16 March 2021)];2020 Available online: https://covid19.who.int/
-
- Huang A.T., Garcia-Carreras B., Hitchings M.D.T., Yang B., Katzelnick L.C., Rattigan S.M., Borgert B.A., Moreno C.A., Solomon B.D., Rodriguez-Barraquer I., et al. A systematic review of antibody mediated immunity to coronaviruses: Antibody kinetics, correlates of protection, and association of antibody responses with severity of disease. medRxiv. 2020 doi: 10.1101/2020.04.14.20065771. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
