

Chondrosarcoma-from Molecular Pathology to Novel Therapies
- PMID: 34069269
- PMCID: PMC8155983
- DOI: 10.3390/cancers13102390
Chondrosarcoma-from Molecular Pathology to Novel Therapies
Abstract
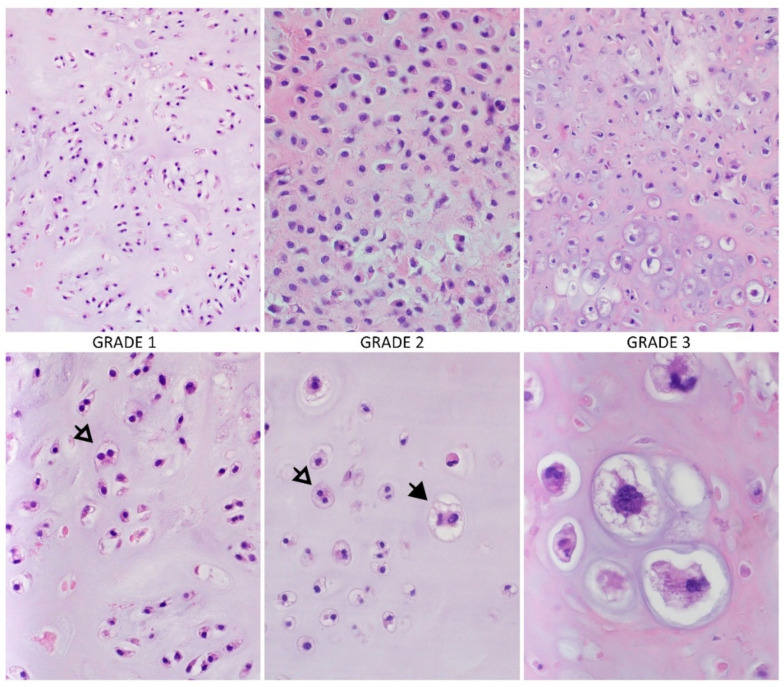
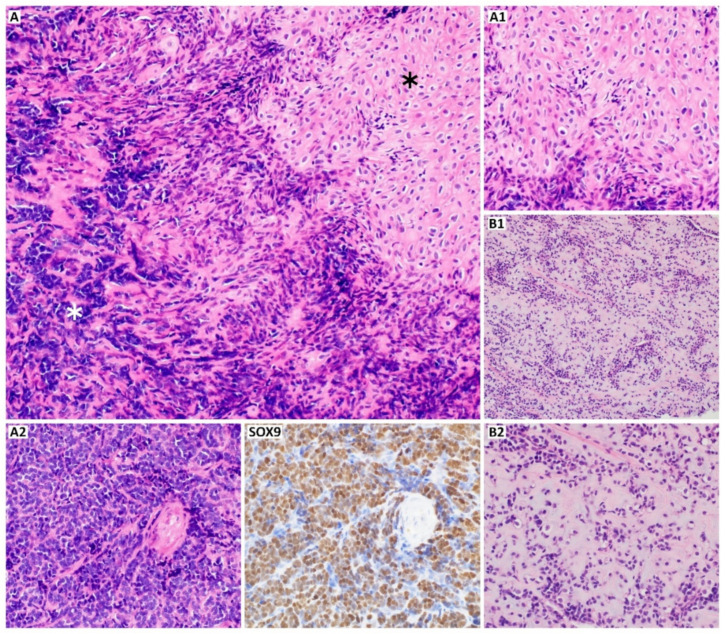
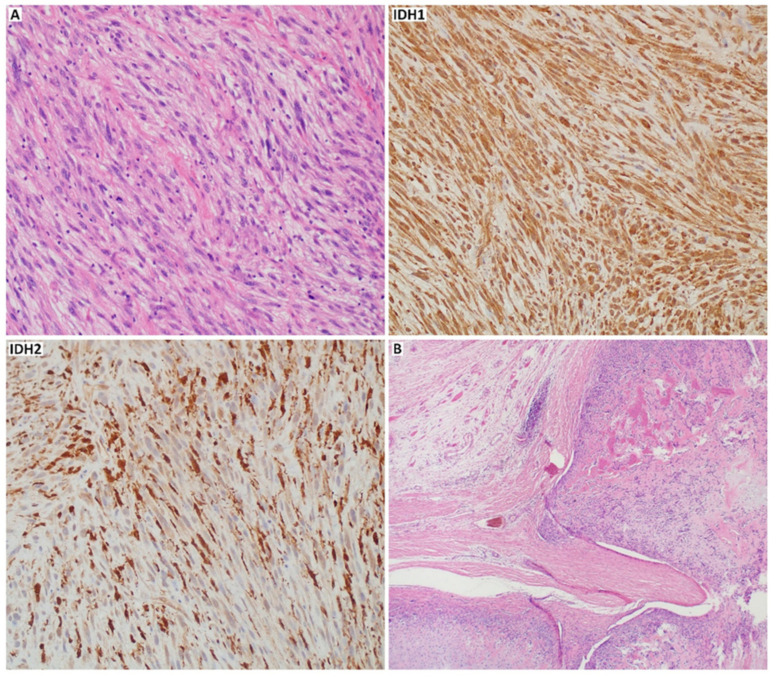
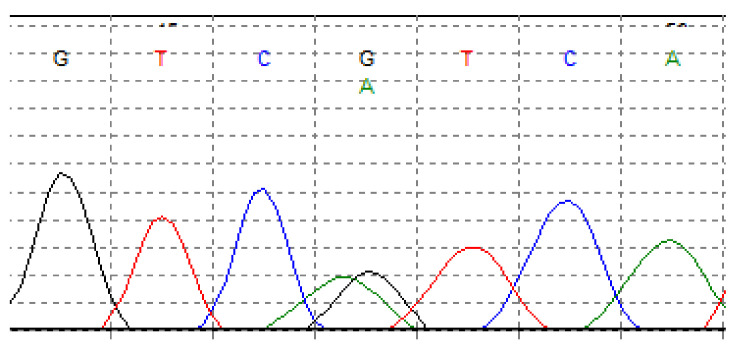
Chondrosarcoma (CHS) is the second most common primary malignant bone sarcoma. Overall survival and prognosis of this tumor are various and often extreme, depending on histological grade and tumor subtype. CHS treatment is difficult, and surgery remains still the gold standard due to the resistance of this tumor to other therapeutic options. Considering the role of differentiation of CHS subtypes and the need to develop new treatment strategies, in this review, we introduced a multidisciplinary characterization of CHS from its pathology to therapies. We described the morphology of each subtype with the role of immunohistochemical markers in diagnostics of CHS. We also summarized the most frequently mutated genes and genome regions with altered pathways involved in the pathology of this tumor. Subsequently, we discussed imaging methods and the role of currently used therapies, including surgery and the limitations of chemo and radiotherapy. Finally, in this review, we presented novel targeted therapies, including those at ongoing clinical trials, which can be a potential future target in designing new therapeutics for patients with CHS.
Keywords: chondrosarcoma; diagnostic markers; pathology; therapies.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
