

Artificial Intelligence Applications to Improve the Treatment of Locally Advanced Non-Small Cell Lung Cancers
- PMID: 34069307
- PMCID: PMC8156328
- DOI: 10.3390/cancers13102382
Artificial Intelligence Applications to Improve the Treatment of Locally Advanced Non-Small Cell Lung Cancers
Abstract
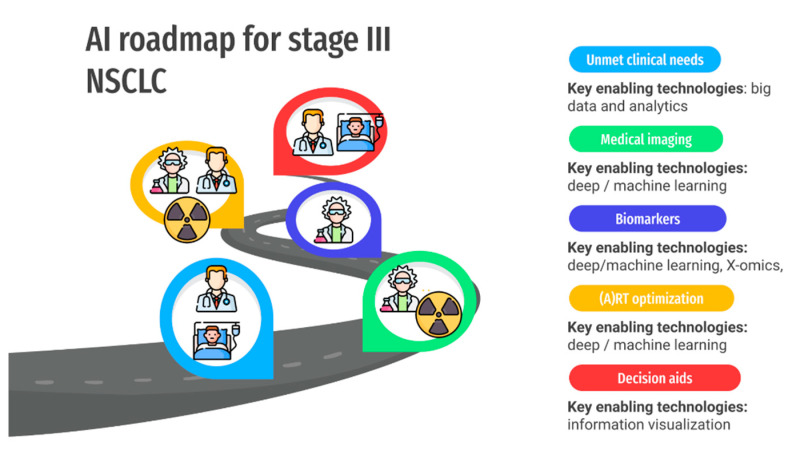
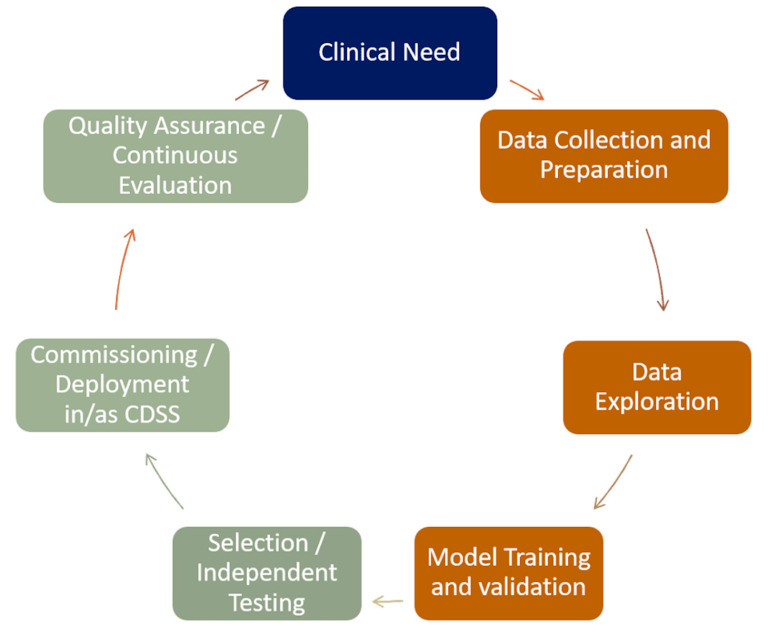
Locally advanced non-small cell lung cancer patients represent around one third of newly diagnosed lung cancer patients. There remains a large unmet need to find treatment strategies that can improve the survival of these patients while minimizing therapeutical side effects. Increasing the availability of patients' data (imaging, electronic health records, patients' reported outcomes, and genomics) will enable the application of AI algorithms to improve therapy selections. In this review, we discuss how artificial intelligence (AI) can be integral to improving clinical decision support systems. To realize this, a roadmap for AI must be defined. We define six milestones involving a broad spectrum of stakeholders, from physicians to patients, that we feel are necessary for an optimal transition of AI into the clinic.
Keywords: artificial intelligence; clinical decision aids; deep learning; lung cancers; radiomics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
