

Association of Perioperative Regional Analgesia with Postoperative Patient-Reported Pain Outcomes and Opioid Requirements: Comparing 22 Different Surgical Groups in 23,911 Patients from the QUIPS Registry
- PMID: 34069496
- PMCID: PMC8160876
- DOI: 10.3390/jcm10102194
Association of Perioperative Regional Analgesia with Postoperative Patient-Reported Pain Outcomes and Opioid Requirements: Comparing 22 Different Surgical Groups in 23,911 Patients from the QUIPS Registry
Abstract
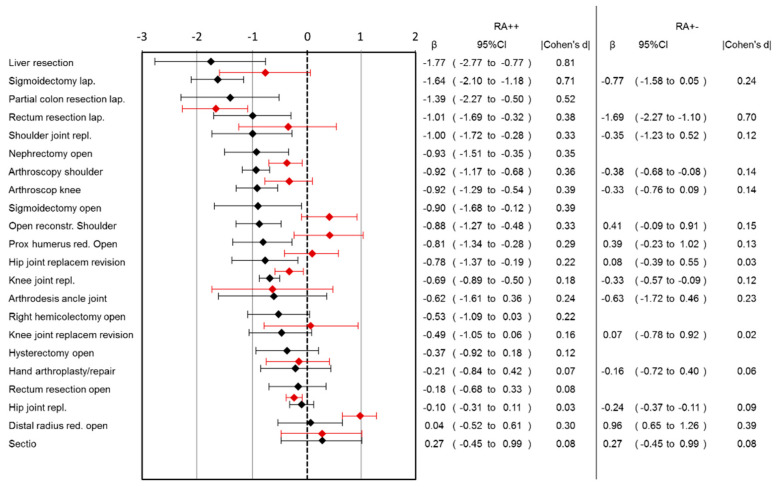
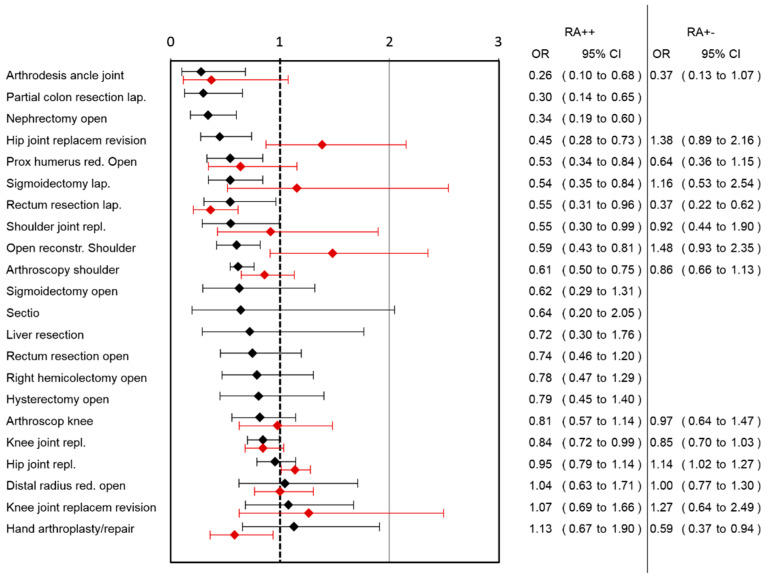
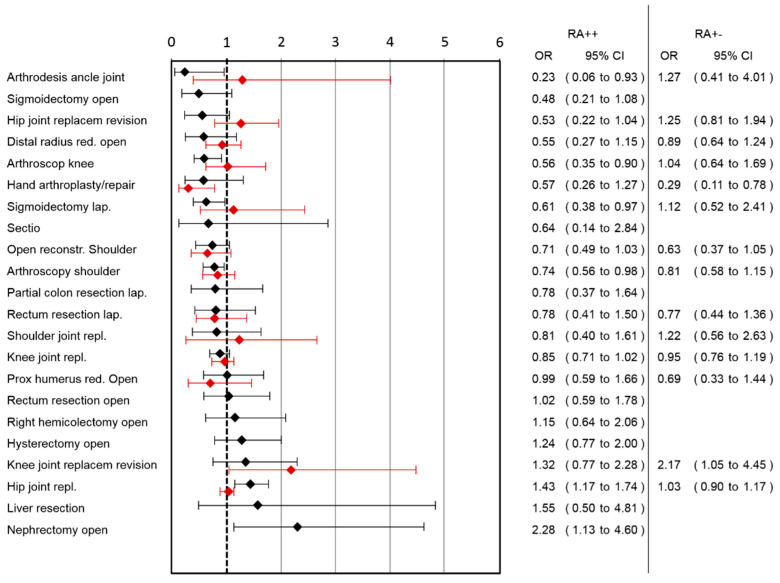
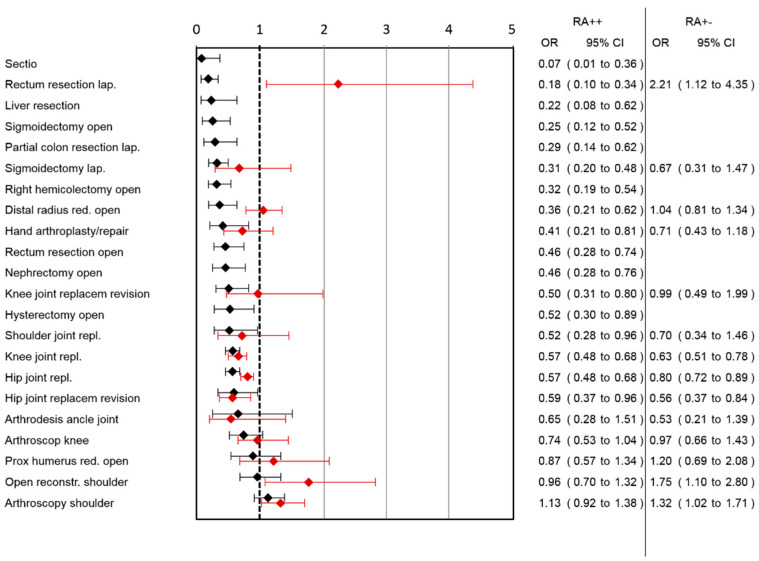
(1) Background: In many surgical procedures, regional analgesia (RA) techniques are associated with improved postoperative analgesia compared to systemic pain treatment. As continuous RA requires time and experienced staff, it would be helpful to identify settings in which continuous RA has the largest benefit. (2) Methods: On the basis of 23,911 data sets from 179 German and Austrian hospitals, we analyzed the association of perioperative RA with patient-reported pain intensity, functional impairment of movement, nausea and opioid use for different surgeries. Regression analyses adjusted for age, sex and preoperative pain were performed for each surgery and the following groups: patients receiving continuous RA (surgery and ward; RA++), RA for surgery only (RA+-) and patients receiving no RA (RA--). (3) Results: Lower pain scores in the RA++ compared to the RA-- group were observed in 13 out of 22 surgeries. There was no surgery where pain scores for RA++ were higher than for RA--. If maximal pain, function and side effects were combined, the largest benefit of continuous RA (RA++) was observed in laparoscopic colon and sigmoid surgery, ankle joint arthrodesis, revision (but not primary) surgery of hip replacement, open nephrectomy and shoulder surgery. The benefit of RA+- was lower than that of RA++. (4) Discussion: The additional benefit of RA for the mentioned surgeries is larger than in many other surgeries in clinical routine. The decision to use RA in a given surgery should be based on the expected pain intensity without RA and its additional benefits.
Keywords: RA; acute pain; functional impairment; opioid consumption; pain management; postoperative pain; regional anesthesia.
Conflict of interest statement
All authors except Winfried Meißner declare no conflict of interest. Winfried Meißner reports grants and personal fees from Grünenthal, grants from Pfizer, personal fees from TAD, personal fees from BioQPharm, personal fees from Bionorica, personal fees from Kyowa, personal fees from Northern Swan, grants from Mundipharma, personal fees from Tilray. All are outside the submitted work.
Figures
References
-
- Wu C.L., Cohen S.R., Richman J.M., Rowlingson A.J., Courpas G.E., Cheung K., Lin E.E., Liu S.S. Efficacy of postoperative patient-controlled and continuous infusion epidural analgesia versus intravenous patient-controlled analgesia with opioids—A meta-analysis. Anesthesiology. 2005;103:1079–1088. doi: 10.1097/00000542-200511000-00023. - DOI - PubMed
-
- Joshi G.P., Bonnet F., Shah R., Wilkinson R.C., Camu F., Fischer B., Neugebauer E.A.M., Rawal N., Schug S.A., Simanski C., et al. A systematic review of randomized trials evaluating regional techniques for postthoracotomy analgesia. Anesth. Analg. 2008;107:1026–1040. doi: 10.1213/01.ane.0000333274.63501.ff. - DOI - PubMed
-
- Chou R., Gordon D.B., de Leon-Casasola O.A., Rosenberg J.M., Bickler S., Brennan T.J., Carter T., Cassidy C.L., Chittenden E.H., Degenhardt E., et al. Management of postoperative pain: A clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council (vol 17, pg 131, 2016) J. Pain. 2016;17:948. doi: 10.1016/j.jpain.2016.05.007. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials
