

Exploring the Complementarity of Pancreatic Ductal Adenocarcinoma Preclinical Models
- PMID: 34069519
- PMCID: PMC8161239
- DOI: 10.3390/cancers13102473
Exploring the Complementarity of Pancreatic Ductal Adenocarcinoma Preclinical Models
Abstract
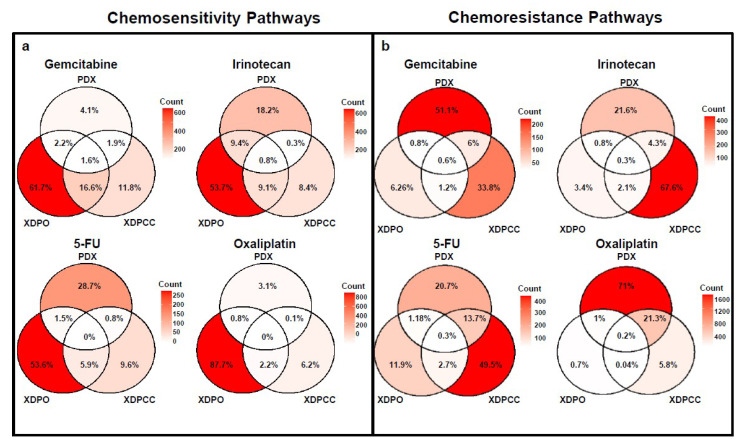
Purpose: Compare pancreatic ductal adenocarcinoma (PDAC), preclinical models, by their transcriptome and drug response landscapes to evaluate their complementarity. Experimental Design: Three paired PDAC preclinical models-patient-derived xenografts (PDX), xenograft-derived pancreatic organoids (XDPO) and xenograft-derived primary cell cultures (XDPCC)-were derived from 20 patients and analyzed at the transcriptomic and chemosensitivity level. Transcriptomic characterization was performed using the basal-like/classical subtyping and the PDAC molecular gradient (PAMG). Chemosensitivity for gemcitabine, irinotecan, 5-fluorouracil and oxaliplatin was established and the associated biological pathways were determined using independent component analysis (ICA) on the transcriptome of each model. The selection criteria used to identify the different components was the chemosensitivity score (CSS) found for each drug in each model. Results: PDX was the most dispersed model whereas XDPO and XDPCC were mainly classical and basal-like, respectively. Chemosensitivity scoring determines that PDX and XDPO display a positive correlation for three out of four drugs tested, whereas PDX and XDPCC did not correlate. No match was observed for each tumor chemosensitivity in the different models. Finally, pathway analysis shows a significant association between PDX and XDPO for the chemosensitivity-associated pathways and PDX and XDPCC for the chemoresistance-associated pathways. Conclusions: Each PDAC preclinical model possesses a unique basal-like/classical transcriptomic phenotype that strongly influences their global chemosensitivity. Each preclinical model is imperfect but complementary, suggesting that a more representative approach of the clinical reality could be obtained by combining them. Translational Relevance: The identification of molecular signatures that underpin drug sensitivity to chemotherapy in PDAC remains clinically challenging. Importantly, the vast majority of studies using preclinical in vivo and in vitro models fail when transferred to patients in a clinical setting despite initially promising results. This study presents for the first time a comparison between three preclinical models directly derived from the same patients. We show that their applicability to preclinical studies should be considered with a complementary focus, avoiding tumor-based direct extrapolations, which might generate misleading conclusions and consequently the overlook of clinically relevant features.
Keywords: chemosensitivity prediction; in vitro models; in vivo models; pancreatic cancer; personalized medicine.
Conflict of interest statement
N.F. (Nicolas Fraunhoffer), J.I. and N.J.D. have a pending patent entitled “Simple transcriptomic signatures to determine chemosensitivity for pancreatic ductal adenocarcinoma”. C.M. (Caroline Mignard) and O.D. are employees of Oncodesign. C.M. (Colin McGuckin) and N.F. (Nico Forraz) are employees of CTIBIOTECH. S.B. is employees of Ipsen Innovation. All other authors declare no competing interests.
Figures




References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
