

Treatment of Unstable Occipital Condylar Fractures in Children-A STROBE-Compliant Investigation
- PMID: 34070410
- PMCID: PMC8228604
- DOI: 10.3390/medicina57060530
Treatment of Unstable Occipital Condylar Fractures in Children-A STROBE-Compliant Investigation
Abstract
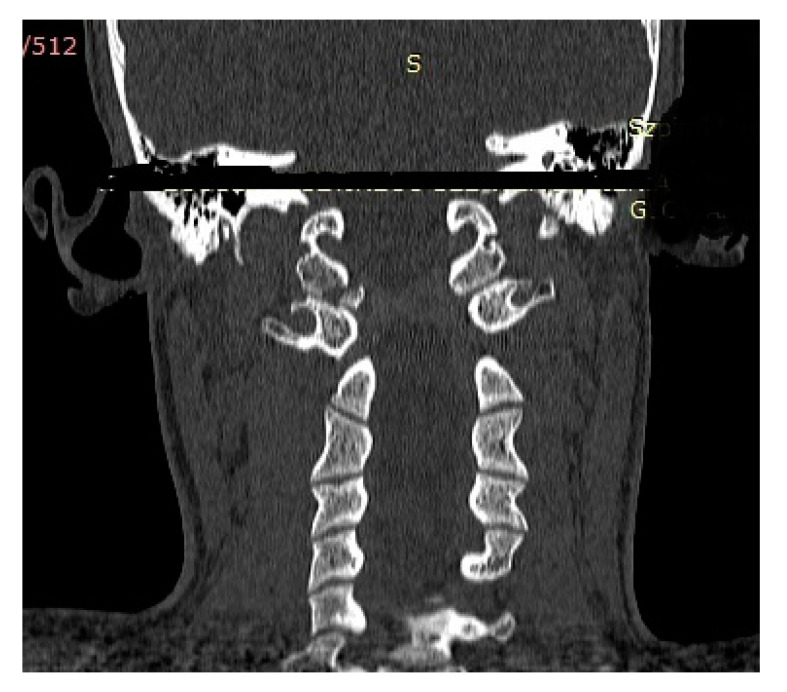
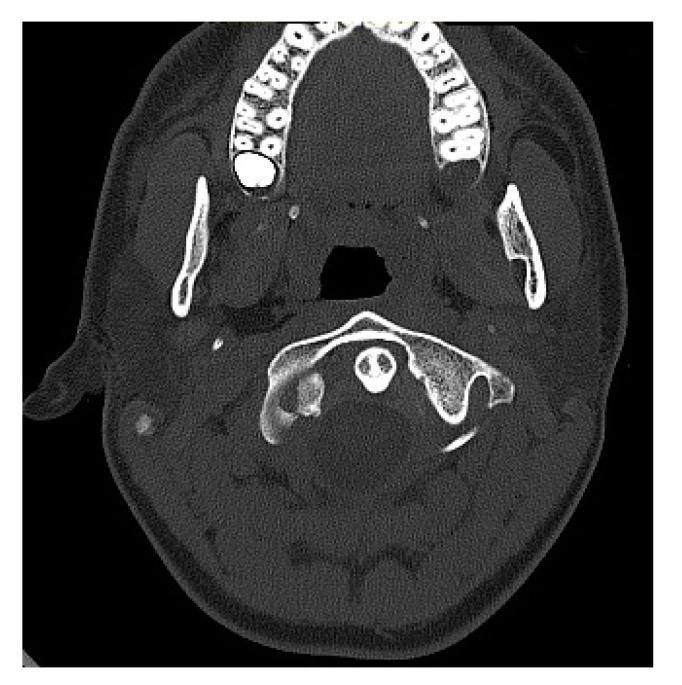
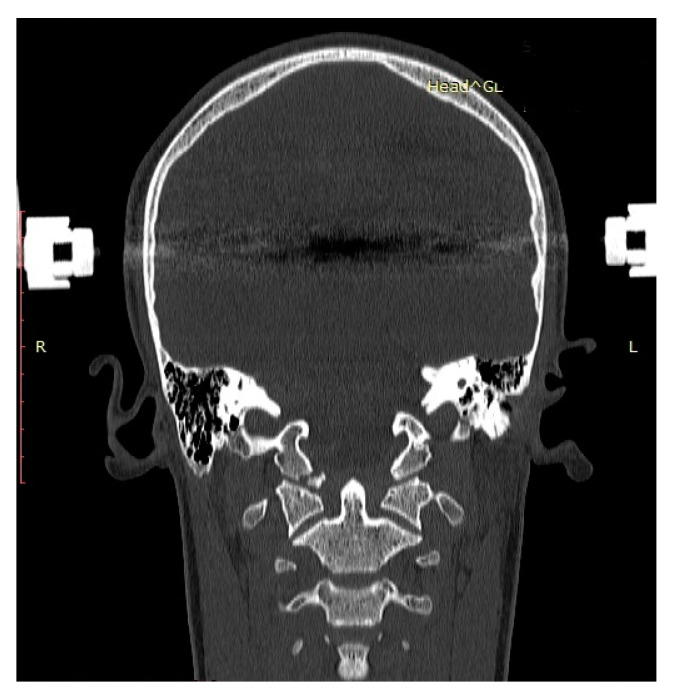
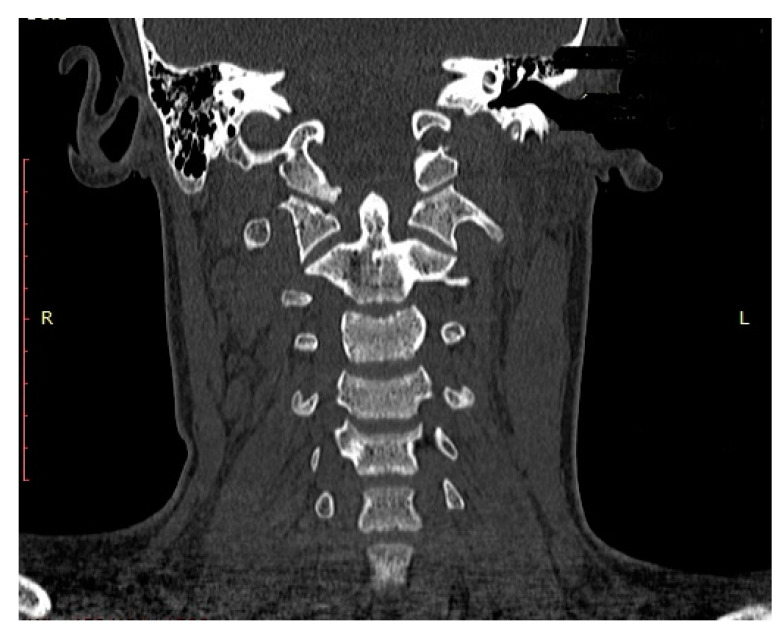
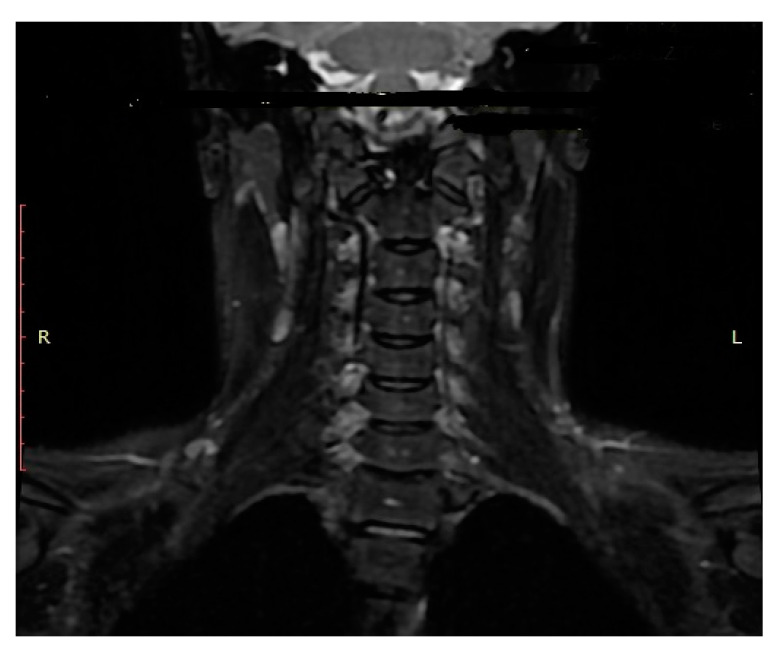
Background and objectives: Occipital condyle fractures (OCF) occur rarely in children. The choice of treatment is based on the Anderson-Montesano and Tuli classification systems. We evaluated the outcome of unstable OCF in children and adolescents after halo-vest therapy. Materials and Methods: We treated 6 pediatric patients for OCF, including 3 patients (2 girls, 1 boy) with unstable OCF. Among the 3 patients with unstable OCF, 2 patients presented with an Anderson-Montesano type III and Tuli type IIB injury, while 1 patient had an Anderson-Montesano type I fracture (Tuli type IIB) accompanied by a C1 fracture. On admission, the children underwent computed tomography (CT) of the head and cervical spine as well as magnetic resonance imaging (MRI) of the cervical spine. We treated the children diagnosed with unstable OCF with halo-vest immobilization. Before removing the halo vest at the end of therapy, we applied the CT and MRI to confirm OCF consolidation. At follow-up, we rated functionality of the craniocervical junction (CCJ) based on the Neck Disability Index (NDI) and Questionnaire Short Form 36 Health Survey (SF-36). Results: All children achieved OCF consolidation after halo-vest therapy for a median of 13.0 weeks (range: 12.5-14.0 weeks). CT and MRI at the end of halo-vest therapy showed no signs of C0/C1 subluxation and confirmed the correct consolidation of OCF. The only complication associated with halo-vest therapy was a superficial infection caused by a halo-vest pin. At follow-up, all children exhibited favorable functionality of the CCJ as documented by the NDI score (median: 3 points; range: 3-11 points) and SF-36 score (median: 91 points; range: 64-96 points). Conclusions: In our small case series, halo-vest therapy resulted in good mid-term outcome in terms of OCF consolidation and CCJ functionality. In pediatric patients with suspected cervical spine injuries, we recommend CT and MRI of the CCJ to establish the diagnosis of OCF and confirm stable fracture consolidation before removing the halo vest.
Keywords: CT; MRI; children; halo vest; occipital condyle fracture.
Conflict of interest statement
ER received funding by the Bob Dickens Research Fellowship in Paediatric Orthopaedic Surgery of the University of Melbourne. The other authors declare no conflict of interest.
Figures
Similar articles
-
Evaluation of using the Anderson-Montesano and the Tuli classifications in pediatric patients with occipital condyle fractures.J Orthop Surg Res. 2021 Jul 13;16(1):449. doi: 10.1186/s13018-021-02463-w. J Orthop Surg Res. 2021. PMID: 34256792 Free PMC article.
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Comparison of outcomes for unstable lower cervical flexion teardrop fractures managed with halo thoracic vest versus anterior corpectomy and plating.Spine (Phila Pa 1976). 2002 Jan 15;27(2):160-6. doi: 10.1097/00007632-200201150-00008. Spine (Phila Pa 1976). 2002. PMID: 11805662
-
Occipital Condyle Fractures in Adolescents.Ortop Traumatol Rehabil. 2015 May-Jun;17(3):219-27. doi: 10.5604/15093492.1162421. Ortop Traumatol Rehabil. 2015. PMID: 26248623
-
A review of halo vest treatment of upper cervical spine injuries.Arch Orthop Trauma Surg. 2001;121(1-2):50-5. doi: 10.1007/s004020000182. Arch Orthop Trauma Surg. 2001. PMID: 11195118 Review.
Cited by
-
Occipital condyle fracture in the pediatric population: A management algorithm and systematic review.J Child Orthop. 2024 Feb 13;18(2):216-228. doi: 10.1177/18632521241229301. eCollection 2024 Apr. J Child Orthop. 2024. PMID: 38567039 Free PMC article. Review.
-
[Pediatric Upper Cervical Spine Injuries: a Systematic Review].Acta Chir Orthop Traumatol Cech. 2025 Mar;92(1):15-20. doi: 10.55095/achot2024/036. Acta Chir Orthop Traumatol Cech. 2025. PMID: 40145585 Czech.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
