

Visual Outcome after Intravitreal Anti-VEGF Therapy for Macular Neovascularisation Secondary to Sorsby's Fundus Dystrophy: A Systematic Review
- PMID: 34070857
- PMCID: PMC8198854
- DOI: 10.3390/jcm10112433
Visual Outcome after Intravitreal Anti-VEGF Therapy for Macular Neovascularisation Secondary to Sorsby's Fundus Dystrophy: A Systematic Review
Abstract
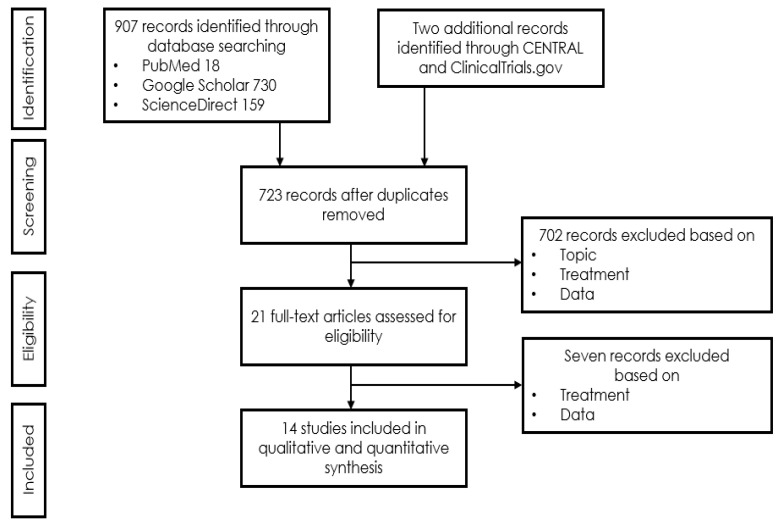
The aim of this paper is to summarise our own and to review published experience regarding the long-term outcome of intravitreal treatment for macular neovascularisation (MNV) secondary to Sorsby's fundus dystrophy (SFD). A systematic literature search using the MeSH terms [Sorsby] and [anti-vascular endothelial growth factor (VEGF)] was conducted in NCBI/PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), ScienceDirect, Google Scholar and ClinicalTrials.gov to identify publications reporting anti-VEGF treatment outcomes in SFD. Treatment outcomes were extracted for this meta-analysis from 14 publications and an own patient reporting a total of 31 cases with a mean follow-up (FU) of 54 months. Both eyes were affected in ten (32.3%) instances. Heterogenous reporting limited the comparability of the outcomes. All papers in common, however, reported satisfied to excellent responses to anti-VEGF therapy if patients were diagnosed and treated immediately after onset of symptoms. Of 20 eyes, for which visual acuity was reported before and after treatment, five worsened and seven improved by more than 1 line, whereas eight eyes maintained their function by end of the follow up, and 11 eyes (55%) maintained a driving vision (Snellen VA ≥ 0.5). Of six eyes with a VA < 0.5, VA improved in one to VA ≥ 0.5, whereas of 14 eyes with an initial VA ≥ 0.5, this dropped to <0.5 despite therapy. In MNV secondary to SFD, the delay between first symptoms and access to anti-VEGF treatment determines subretinal scar formation and thereby, functional prognosis. If treated early, this is generally favourable under regular controls and a consequent anti-VEGF treatment of MNV activity.
Keywords: Sorsby; Sorsby’s fundus dystrophy; anti-VEGF treatment; choroidal neovascularisation; hereditary retinal dystrophy; long-term FU; macular neovascularization; treatment outcome.
Conflict of interest statement
The authors declare no conflict of interest. (Commercial relationships disclosures: Arthur Baston, None; Christin Gerhardt, None; Souska Zandi, None; Justus G. Garweg, AbbVie, Alcon, Chengdu Khanghong, Bayer, Novartis).
Figures

References
-
- Sorsby A., Mason M.E.J., Gardener N. A Fundus Dystrophy with Unusual Features (Late onset and dominant inheritance of a central retinal lesion showing oedema, haemorrhage and exudates developing into generalised choroidal atrophy with massive pigment proliferation) Br. J. Ophthalmol. 1949;33:67–97. doi: 10.1136/bjo.33.2.67. - DOI - PMC - PubMed
-
- Qi J.H., Ebrahem Q., Ali M., Cutler A., Bell B., Prayson N., Sears J., Knauper V., Murphy G., Anand-Apte B. Tissue Inhibitor of Metalloproteinases-3 Peptides Inhibit Angiogenesis and Choroidal Neovascularization in Mice. PLoS ONE. 2013;8:e55667. doi: 10.1371/journal.pone.0055667. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
