

Advances in Multidisciplinary Management of Skull Base Meningiomas
- PMID: 34071391
- PMCID: PMC8198762
- DOI: 10.3390/cancers13112664
Advances in Multidisciplinary Management of Skull Base Meningiomas
Abstract
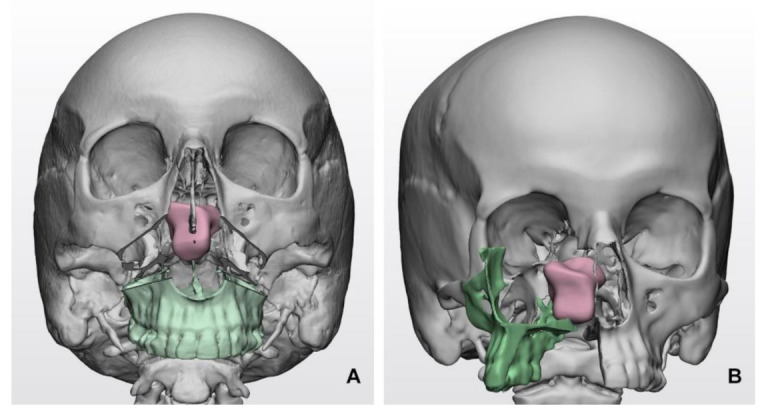
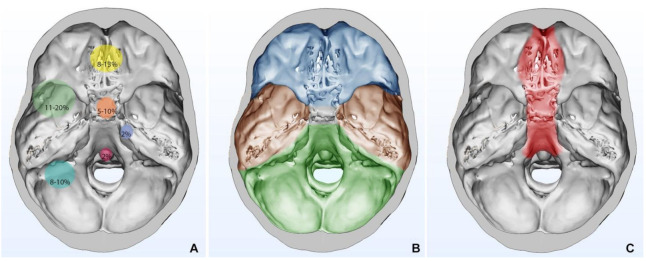
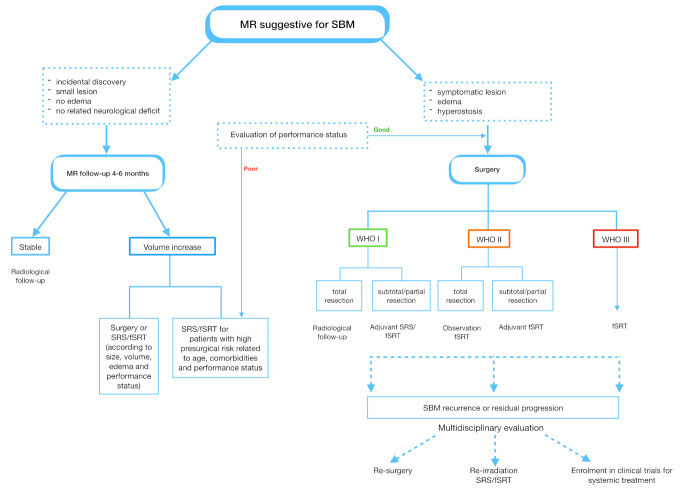
The surgical management of Skull Base Meningiomas (SBMs) has radically changed over the last two decades. Extensive surgery for patients with SBMs represents the mainstream treatment; however, it is often challenging due to narrow surgical corridors and proximity to critical neurovascular structures. Novel surgical technologies, including three-dimensional (3D) preoperative imaging, neuromonitoring, and surgical instruments, have gradually facilitated the surgical resectability of SBMs, reducing postoperative morbidity. Total removal is not always feasible considering a risky tumor location and invasion of surrounding structures and brain parenchyma. In recent years, the use of primary or adjuvant stereotactic radiosurgery (SRS) has progressively increased due to its safety and efficacy in the control of grade I and II meningiomas, especially for small to moderate size lesions. Patients with WHO grade SBMs receiving subtotal surgery can be monitored over time with surveillance imaging. Postoperative management remains highly controversial for grade II meningiomas, and depends on the presence of residual disease, with optional upfront adjuvant radiation therapy or close surveillance imaging in cases with total resection. Adjuvant radiation is strongly recommended in patients with grade III tumors. Although the currently available chemotherapy or targeted therapies available have a low efficacy, the molecular profiling of SBMs has shown genetic alterations that could be potentially targeted with novel tailored treatments. This multidisciplinary review provides an update on the advances in surgical technology, postoperative management and molecular profile of SBMs.
Keywords: 3D virtual planning; radiosurgery; radiotherapy; skull base meningioma; surgery; systemic treatment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Louis D.N., Perry A., Reifenberger G., von Deimling A., Figarella-Branger D., Cavenee W.K., Ohgaki H., Wiestler O.D., Kleihues P., Ellison D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A Summary. Acta Neuropathol. 2016;131:803–820. doi: 10.1007/s00401-016-1545-1. - DOI - PubMed
-
- Flood L.M. In: Meningiomas of the Skull Base: Treatment Nuances in Contemporary Neurosurgery. Cappabianca P., Solari D., editors. Thieme; Stuttgart, NY, USA: 2018.
Publication types
LinkOut - more resources
Full Text Sources
