

Emerging Insights into Targeted Therapy-Tolerant Persister Cells in Cancer
- PMID: 34071428
- PMCID: PMC8198243
- DOI: 10.3390/cancers13112666
Emerging Insights into Targeted Therapy-Tolerant Persister Cells in Cancer
Abstract
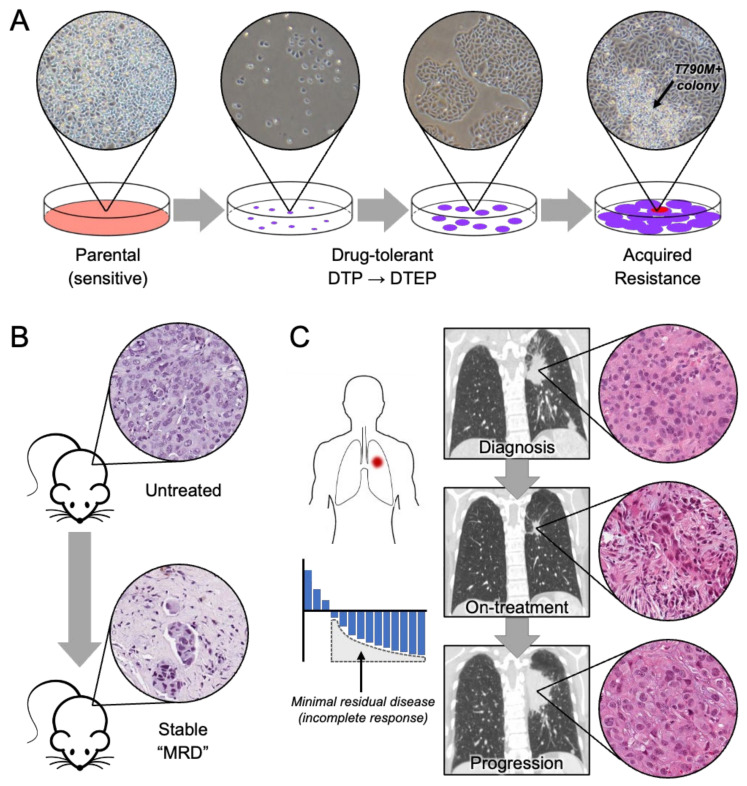
Drug resistance is perhaps the greatest challenge in improving outcomes for cancer patients undergoing treatment with targeted therapies. It is becoming clear that "persisters," a subpopulation of drug-tolerant cells found in cancer populations, play a critical role in the development of drug resistance. Persisters are able to maintain viability under therapy but are typically slow cycling or dormant. These cells do not harbor classic drug resistance driver alterations, and their partial resistance phenotype is transient and reversible upon removal of the drug. In the clinic, the persister state most closely corresponds to minimal residual disease from which relapse can occur if treatment is discontinued or if acquired drug resistance develops in response to continuous therapy. Thus, eliminating persister cells will be crucial to improve outcomes for cancer patients. Using lung cancer targeted therapies as a primary paradigm, this review will give an overview of the characteristics of drug-tolerant persister cells, mechanisms associated with drug tolerance, and potential therapeutic opportunities to target this persister cell population in tumors.
Keywords: acquired drug resistance; drug-tolerant persisters; targeted therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Lynch T.J., Bell D.W., Sordella R., Gurubhagavatula S., Okimoto R.A., Brannigan B.W., Harris P.L., Haserlat S.M., Supko J.G., Haluska F.G., et al. Activating Mutations in the Epidermal Growth Factor Receptor Underlying Responsiveness of Non–Small-Cell Lung Cancer to Gefitinib. N. Engl. J. Med. 2004;350:2129–2139. doi: 10.1056/NEJMoa040938. - DOI - PubMed
-
- Mok T., Camidge D.R., Gadgeel S.M., Rosell R., Dziadziuszko R., Kim D.W., Perol M., Ou S.I., Ahn J.S., Shaw A.T., et al. Updated overall survival and final progression-free survival data for patients with treatment-naive advanced ALK-positive non-small-cell lung cancer in the ALEX study. Ann. Oncol. 2020;31:1056–1064. doi: 10.1016/j.annonc.2020.04.478. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
