

Polycystic Ovary Syndrome in Insulin-Resistant Adolescents with Obesity: The Role of Nutrition Therapy and Food Supplements as a Strategy to Protect Fertility
- PMID: 34071499
- PMCID: PMC8228678
- DOI: 10.3390/nu13061848
Polycystic Ovary Syndrome in Insulin-Resistant Adolescents with Obesity: The Role of Nutrition Therapy and Food Supplements as a Strategy to Protect Fertility
Abstract
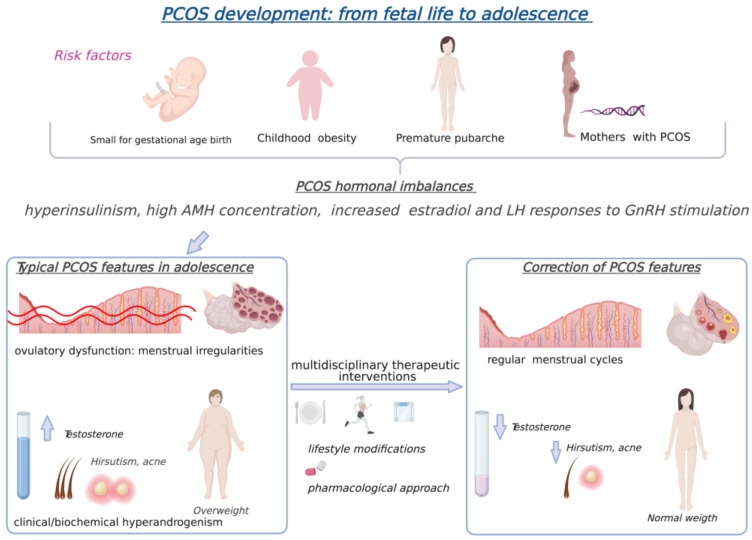
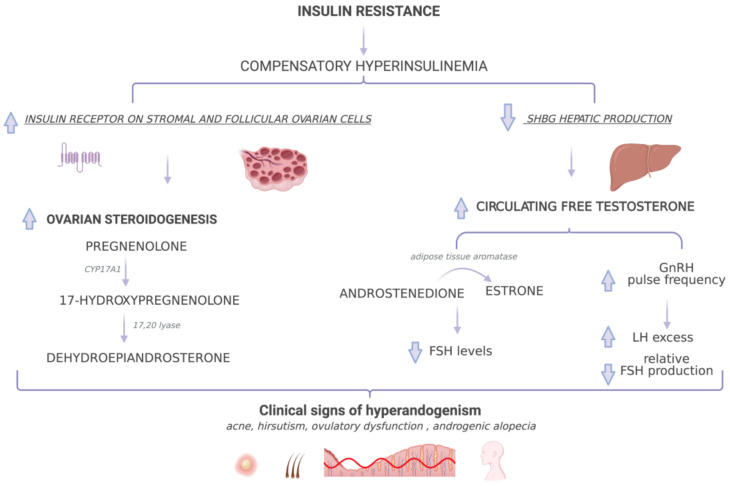
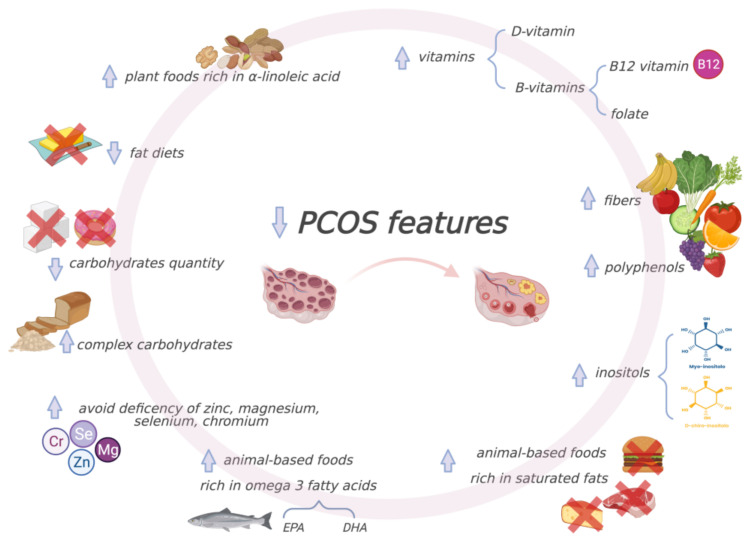
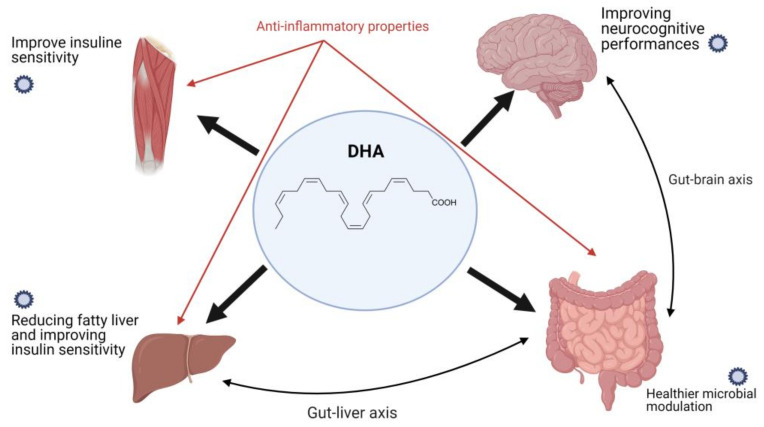
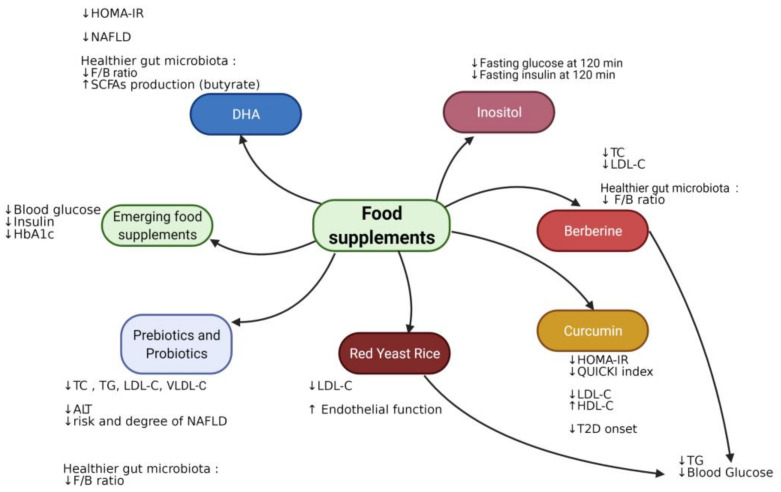
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder in young reproductive-aged women. PCOS is often associated with obesity and impairs reproductive health. Even though several theories have been proposed to explain the pathogenic mechanism of PCOS, the role of insulin resistance (IR) as a key etiological component, independently of (but amplified by) obesity, is well recognized. The consequent hyperinsulinemia activates excessive ovarian androgen production, leading to PCOS. Additionally, the state of chronic inflammation related to obesity impacts ovarian physiology due to insulin sensitivity impairment. The first-line treatment for adolescents with obesity and PCOS includes lifestyle changes; personalized dietary interventions; and, when needed, weight loss. Medical nutrition therapy (MNT) and the use of specific food supplements in these patients aim at improving symptoms and signs, including insulin resistance and metabolic and reproductive functions. The purpose of this narrative review is to present and discuss PCOS in adolescents with obesity, its relationship with IR and the role of MNT and food supplements in treatment. Appropriate early dietary intervention for the management of adolescents with obesity and PCOS should be considered as the recommended approach to restore ovulation and to protect fertility.
Keywords: adolescents; diet; fertility; food supplements; nutrition; obesity; polycystic ovary syndrome.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
