

Evidence-Based Recommendations for an Optimal Prenatal Supplement for Women in the U.S., Part Two: Minerals
- PMID: 34071548
- PMCID: PMC8229801
- DOI: 10.3390/nu13061849
Evidence-Based Recommendations for an Optimal Prenatal Supplement for Women in the U.S., Part Two: Minerals
Abstract
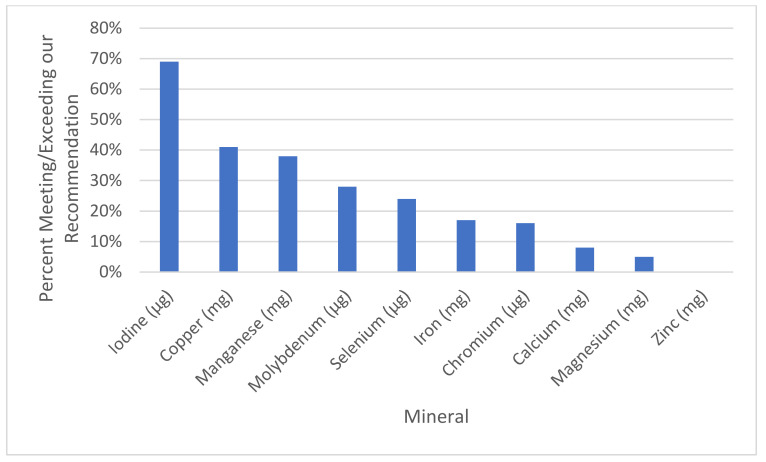
The levels of many essential minerals decrease during pregnancy if un-supplemented, including calcium, iron, magnesium, selenium, zinc, and possibly chromium and iodine. Sub-optimal intake of minerals from preconception through pregnancy increases the risk of many pregnancy complications and infant health problems. In the U.S., dietary intake of minerals is often below the Recommended Dietary Allowance (RDA), especially for iodine and magnesium, and 28% of women develop iron deficiency anemia during their third trimester. The goal of this paper is to propose evidence-based recommendations for the optimal level of prenatal supplementation for each mineral for most women in the United States. Overall, the evidence suggests that optimal mineral supplementation can significantly reduce a wide range of pregnancy complications (including anemia, gestational hypertension, gestational diabetes, hyperthyroidism, miscarriage, and pre-eclampsia) and infant health problems (including anemia, asthma/wheeze, autism, cerebral palsy, hypothyroidism, intellectual disability, low birth weight, neural tube defects, preterm birth, rickets, and wheeze). An evaluation of 180 commercial prenatal supplements found that they varied widely in mineral content, often contained only a subset of essential minerals, and the levels were often below our recommendations. Therefore, there is a need to establish recommendations on the optimal level of mineral supplementation during pregnancy.
Keywords: calcium; chromium; iron; magnesium; minerals; pregnancy; selenium; supplements.
Conflict of interest statement
JBA is the Chair of the Scientific Advisory Board of the Neurological Health Foundation (NHF), Chair of the NHF Task Force on Pregnancy-Safe Products, co-leader of the Scientific Advisory Board of the Autism Research Institute, member of the Scientific Advisory Board for an autism study of Finch Therapeutics, President of the Autism Nutrition Research Center, President of Autism Diagnostics, President of Autism Therapeutics, and President of the Autism Society of Greater Phoenix. He has received grant funding from the Department of Defense, Finch Therapeutics, Autism Research Institute, Autism Nutrition Research Center, and BHARE Foundation. He is a consultant for Finch Therapeutics and Healthy Nest, and in the latter case, he led the development of their prenatal supplement. He has patents/pending patents licensed to Finch Therapeutics and Autism Diagnostics.
Figures

References
-
- Pettifor J.M. Vitamin D &/or calcium deficiency rickets in infants & children: A global perspective. Indian J. Med. Res. 2008;127:245–249. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
