

Association of Health Insurance Status with Outcomes of Sepsis in Adult Patients: A Retrospective Cohort Study
- PMID: 34072210
- PMCID: PMC8198413
- DOI: 10.3390/ijerph18115777
Association of Health Insurance Status with Outcomes of Sepsis in Adult Patients: A Retrospective Cohort Study
Abstract
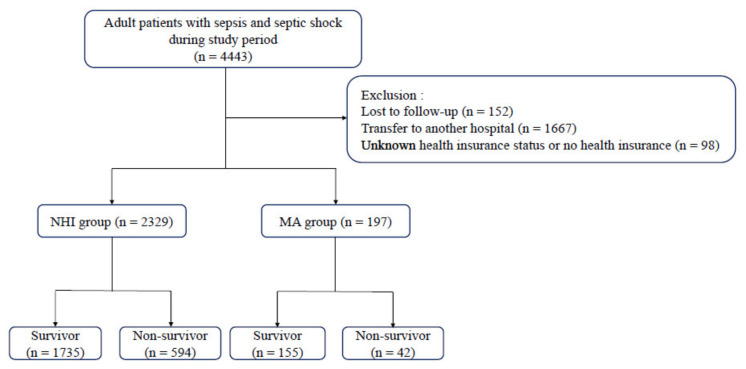
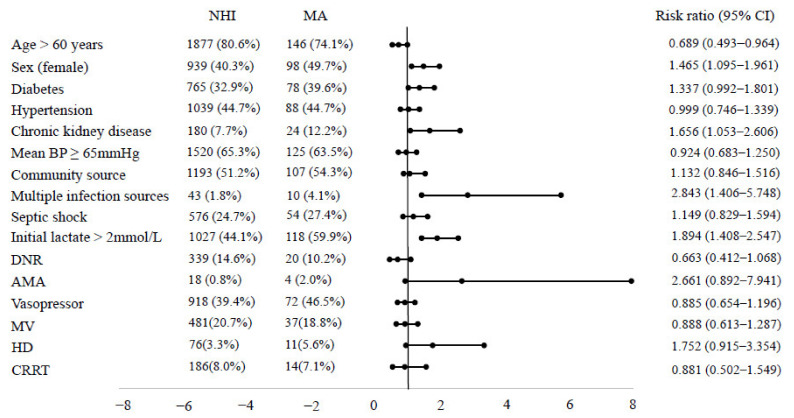
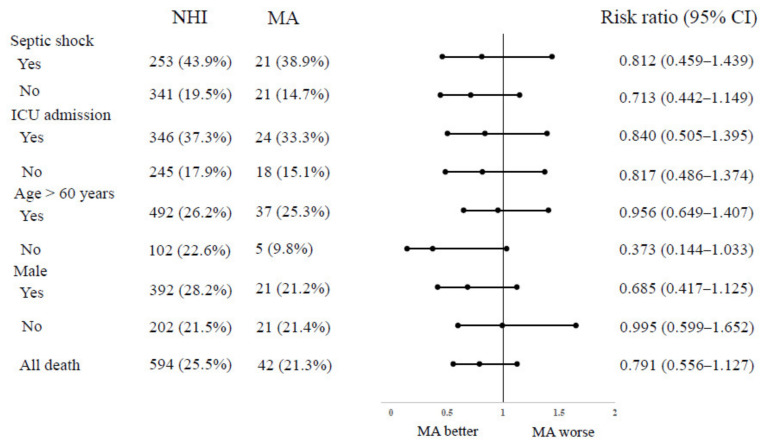
(1) Background: Sepsis is a life-threatening disease, and various demographic and socioeconomic factors affect outcomes in sepsis. However, little is known regarding the potential association between health insurance status and outcomes of sepsis in Korea. We evaluated the association of health insurance and clinical outcomes in patients with sepsis. (2) Methods: Prospective cohort data of adult patients with sepsis and septic shock from March 2016 to December 2018 in three hospitals were retrospectively analyzed. We categorized patients into two groups according to their health insurance status: National Health Insurance (NHI) and Medical Aid (MA). The primary end point was in-hospital mortality. The multivariate logistic regression model and propensity score matching were used. (3) Results: Of a total of 2526 eligible patients, 2329 (92.2%) were covered by NHI, and 197 (7.8%) were covered by MA. The MA group had fewer males, more chronic kidney disease, more multiple sources of infection, and more patients with initial lactate > 2 mmol/L. In-hospital, 28-day, and 90-day mortality were not significantly different between the two groups and in-hospital mortality was not different in the subgroup analysis. Furthermore, health insurance status was not independently associated with in-hospital mortality in multivariate analysis and was not associated with survival outcomes in the propensity score-matched cohort. (4) Conclusions: Our propensity score-matched cohort analysis demonstrated that there was no significant difference in in-hospital mortality by health insurance status in patients with sepsis.
Keywords: health insurance; mortality; outcome; sepsis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Rhodes A., Evans L.E., Alhazzani W., Levy M.M., Antonelli M., Ferrer R., Kumar A., Sevransky J.E., Sprung C.L., Nunnally M.E., et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43:304–377. doi: 10.1007/s00134-017-4683-6. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
