

Electrocardiographic Versus Echocardiographic Left Ventricular Hypertrophy in Severe Aortic Stenosis
- PMID: 34072214
- PMCID: PMC8198672
- DOI: 10.3390/jcm10112362
Electrocardiographic Versus Echocardiographic Left Ventricular Hypertrophy in Severe Aortic Stenosis
Abstract
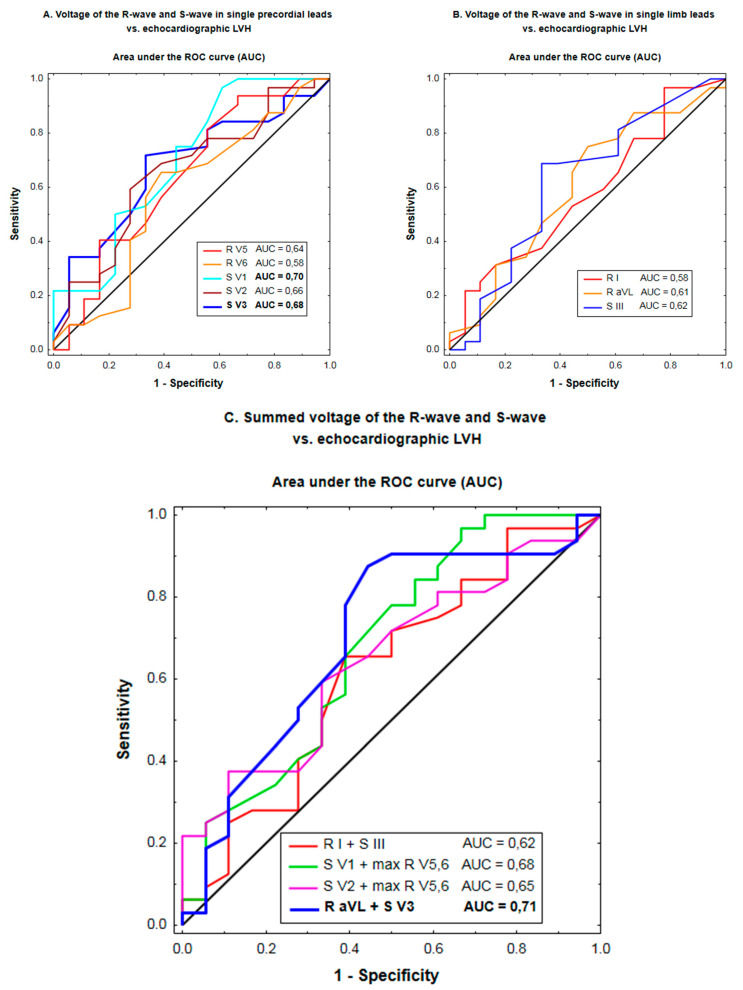
Although ECG used to be a traditional method to detect left ventricular hypertrophy (LVH), its importance has decreased over the years and echocardiography has emerged as a routine technique to diagnose LVH. Intriguingly, an independent negative prognostic effect of the "electrical" LVH (i.e., by ECG voltage criteria) beyond echocardiographic LVH was demonstrated both in hypertension and aortic stenosis (AS), the most prevalent heart valve disorder. Our aim was to estimate associations of the ECG-LVH voltage criteria with echocardiographic LVH and indices of AS severity. We retrospectively manually analyzed ECG tracings of 50 patients hospitalized in our center for severe isolated aortic stenosis, including 32 subjects with echocardiographic LVH. The sensitivity of single traditional ECG-LVH criteria in detecting echocardiographic LVH was 9-34% and their respective specificity averaged 78-100%. The ability to predict echocardiographic LVH was higher for S-waves than R-waves (mean area under the receiver operating curve (AUC): 0.62-0.70 vs. 0.58-0.65). Among combinations of R- and S-waves, the discriminating ability was highest for the Cornell voltage (AUC: 0.71) compared to the Sokolow-Lyon, Romhilt and Gubner-Ungerleider voltage (AUC: 0.62-0.68). By multiple regression, peak aortic pressure gradient was positively related to the Sokolow-Lyon (β = 1.7 ± 0.5, p = 0.002) and Romhilt voltage (β = 1.3 ± 0.5, p = 0.01), but not Cornell (0.5 ± 0.3, p = 0.2) or Gubner-Ungerleider voltage (β = 0.0 ± 0.5, p > 0.9), regardless of LV mass index. In conclusion, echocardiographic LVH and stenosis severity appear to have distinct associations with traditional ECG-LVH criteria in AS. A moderate diagnostic superiority of the Cornell voltage criterion with regard to anatomic LVH might result from its unique ability to include depolarization vectors in both the frontal and horizontal plane with consequent lesser sensitivity to the confounding effect of obesity.
Keywords: aortic stenosis; echocardiography; electrocardiography; left ventricular hypertrophy.
Conflict of interest statement
The authors declare no conflict of interest. The funder of the APC had no role in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript or in the decision to publish the results.
Figures
Similar articles
-
Diagnostic Ability of Peguero-Lo Presti Electrocardiographic Left Ventricular Hypertrophy Criterion in Severe Aortic Stenosis.J Clin Med. 2021 Jun 28;10(13):2864. doi: 10.3390/jcm10132864. J Clin Med. 2021. PMID: 34203345 Free PMC article.
-
The relationship between electrocardiographic left ventricular hypertrophy criteria and echocardiographic mass in patients undergoing transcatheter aortic valve replacement.J Electrocardiol. 2015 Jul-Aug;48(4):630-6. doi: 10.1016/j.jelectrocard.2015.03.008. Epub 2015 Mar 11. J Electrocardiol. 2015. PMID: 25865909
-
Electrocardiographic criteria for left ventricular hypertrophy in aortic valve stenosis: Correlation with echocardiographic parameters.Ann Noninvasive Electrocardiol. 2019 Sep;24(5):e12645. doi: 10.1111/anec.12645. Epub 2019 Mar 21. Ann Noninvasive Electrocardiol. 2019. PMID: 30896064 Free PMC article.
-
Regression of electrocardiographic left ventricular hypertrophy or strain is associated with lower incidence of cardiovascular morbidity and mortality in hypertensive patients independent of blood pressure reduction - A LIFE review.J Electrocardiol. 2014 Sep-Oct;47(5):630-5. doi: 10.1016/j.jelectrocard.2014.07.003. Epub 2014 Jul 3. J Electrocardiol. 2014. PMID: 25052475 Review.
-
Diagnostic Accuracy of ECG to Detect Left Ventricular Hypertrophy in Patients with Left Bundle Branch Block: A Systematic Review and Meta-analysis.CJC Open. 2023 Aug 30;5(12):971-980. doi: 10.1016/j.cjco.2023.08.010. eCollection 2023 Dec. CJC Open. 2023. PMID: 38204852 Free PMC article. Review.
Cited by
-
Diagnostic Ability of Peguero-Lo Presti Electrocardiographic Left Ventricular Hypertrophy Criterion in Severe Aortic Stenosis.J Clin Med. 2021 Jun 28;10(13):2864. doi: 10.3390/jcm10132864. J Clin Med. 2021. PMID: 34203345 Free PMC article.
-
Electrocardiography versus Echocardiography in Severe Aortic Stenosis with the Consideration of Coexistent Coronary Artery Disease.J Clin Med. 2024 Feb 9;13(4):1013. doi: 10.3390/jcm13041013. J Clin Med. 2024. PMID: 38398326 Free PMC article.
References
-
- Devereux R.B., Bella J., Roman K., Gerdts E., Nieminen M.S., Rokkedal J., Papademetriou V., Wachtell K., Wright J., Paranicas M., et al. Echocardiographic left ventricular geometry in hypertensive patients with electrocardiographic left ventricular hypertrophy: The LIFE Study. Blood Press. 2001;10:74–82. doi: 10.1080/08037050152112050. - DOI - PubMed
-
- Pewsner D., Jüni P., Egger M., Battaglia M., Sundström J., Bachmann L.M. Accuracy of electrocardiography in diagnosis of left ventricular hypertrophy in arterial hypertension: Systematic review. BMJ. 2007;335:711. doi: 10.1136/bmj.39276.636354.AE. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
