

Inappropriate Use of Oral Antithrombotic Combinations in an Outpatient Setting and Associated Risks: A French Nationwide Cohort Study
- PMID: 34072261
- PMCID: PMC8198137
- DOI: 10.3390/jcm10112367
Inappropriate Use of Oral Antithrombotic Combinations in an Outpatient Setting and Associated Risks: A French Nationwide Cohort Study
Abstract
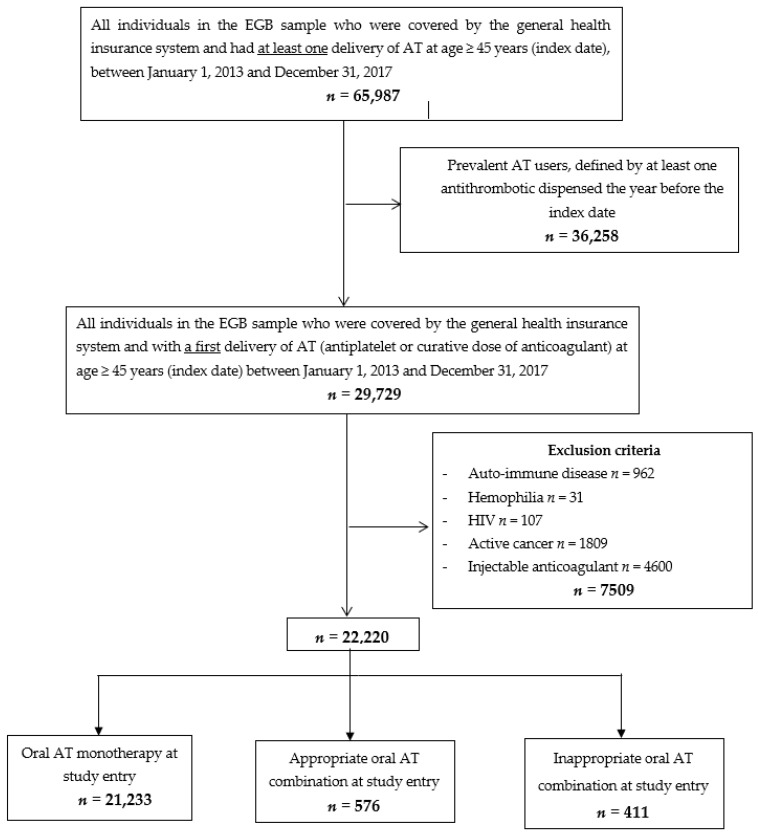
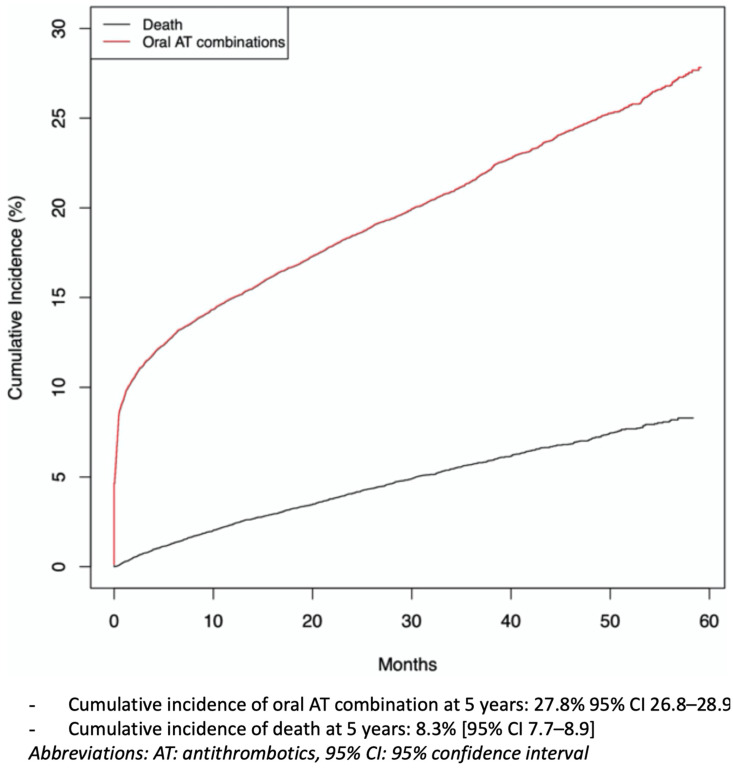
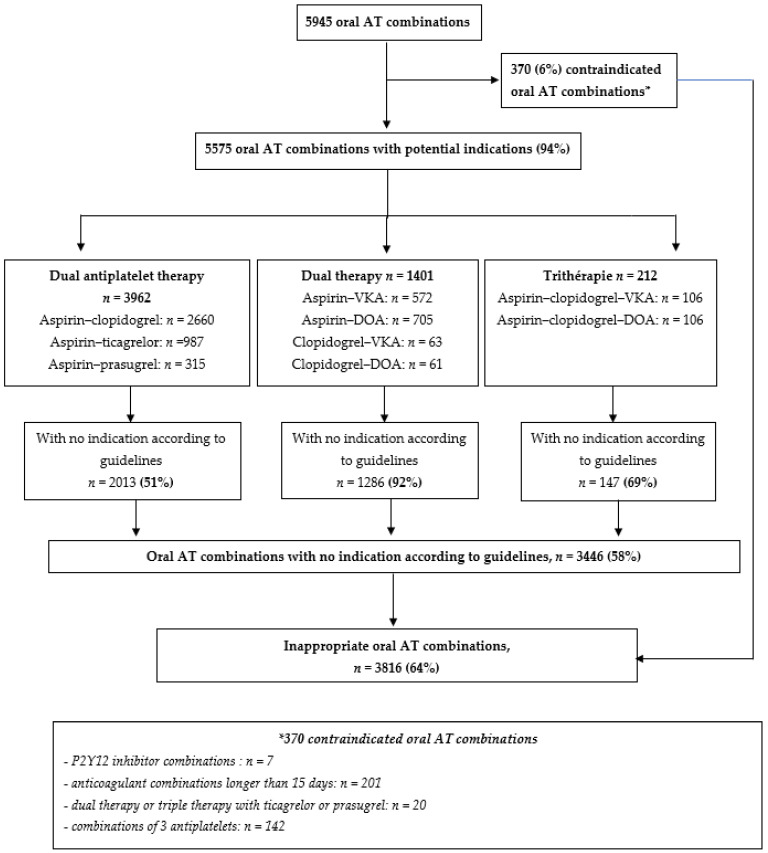
With the increase in prevalence of cardiovascular diseases, multimorbidity, and medical progress, oral antithrombotic (AT) combinations are increasingly prescribed. The aims of this study were to estimate the incidence of oral AT combinations, their appropriateness (defined as indications compliant with guidelines), and the related risk of major bleeding (i.e., leading to hospitalization) or death, among new users. We conducted a 5-year historical cohort study, using the French national healthcare database, including all individuals ≥ 45 years old with a first delivery of oral ATs between 1 January 2013 and 31 December 2017. The cumulative incidence of oral AT combinations was estimated with the Fine and Gray method, taking into account the competitive risk of death. We compared the cumulative incidence of major bleeding according to the type of oral AT treatment initiated at study entry (monotherapy or oral AT combinations). During the study period, 22,220 individuals were included (mean (SD) age 68 (12) years). The cumulative incidence of oral AT combinations at 5 years was 27.8% (95% confidence interval (CI) 26.8-28.9). Overall, 64% of any oral AT combinations did not comply with guidelines. The cumulative incidence of major bleeding and death in the whole cohort at 5 years was 4.1% (95% CI 3.7-4.6) and 10.8% (95% CI 10.1-11.6), respectively. Risk of major bleeding increased among individuals with oral AT combinations versus oral AT monotherapy at study entry (subdistribution hazard ratio sHR: 2.16 (1.01-4.63)); with no difference in terms of death. The use of oral AT combinations among oral AT users is frequent, often inappropriately prescribed, and associated with an increased risk of major bleeding.
Keywords: adverse drug event; antithrombotic combinations; hemorrhage; inappropriate prescribing; vascular diseases.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures
Similar articles
-
Association of NSAID use with risk of bleeding and cardiovascular events in patients receiving antithrombotic therapy after myocardial infarction.JAMA. 2015 Feb 24;313(8):805-14. doi: 10.1001/jama.2015.0809. JAMA. 2015. PMID: 25710657
-
A prescription support-tool for chronic management of oral antithrombotic combinations in adults based on a systematic review of international guidelines.PLoS One. 2019 Feb 14;14(2):e0211695. doi: 10.1371/journal.pone.0211695. eCollection 2019. PLoS One. 2019. PMID: 30763325 Free PMC article.
-
Major Bleeding Rates in Atrial Fibrillation Patients on Single, Dual, or Triple Antithrombotic Therapy.Circulation. 2019 Feb 5;139(6):775-786. doi: 10.1161/CIRCULATIONAHA.118.036248. Circulation. 2019. PMID: 30586754
-
Antiplatelet therapy for stable coronary artery disease in atrial fibrillation patients taking an oral anticoagulant: a nationwide cohort study.Circulation. 2014 Apr 15;129(15):1577-85. doi: 10.1161/CIRCULATIONAHA.113.004834. Epub 2014 Jan 27. Circulation. 2014. PMID: 24470482
-
[Cost-effectiveness analysis of schizophrenic patient care settings: impact of an atypical antipsychotic under long-acting injection formulation].Encephale. 2005 Mar-Apr;31(2):235-46. doi: 10.1016/s0013-7006(05)82390-5. Encephale. 2005. PMID: 15959450 Review. French.
Cited by
-
New Paradigms in Antithrombotic Strategies: A Leap into the Future of Cardiovascular Medicine.J Clin Med. 2022 May 10;11(10):2693. doi: 10.3390/jcm11102693. J Clin Med. 2022. PMID: 35628820 Free PMC article.
-
A qualitative evaluation of barriers and facilitators to a large-scale antithrombotic stewardship intervention in the United States Veterans Healthcare system.Int J Clin Pharm. 2025 Jun 4. doi: 10.1007/s11096-025-01922-2. Online ahead of print. Int J Clin Pharm. 2025. PMID: 40465183
References
-
- Hansen M.L., Sørensen R., Clausen M.T., Fog-Petersen M.L., Raunsø J., Gadsbøll N., Gislason G.H., Folke F., Andersen S.S., Schramm T.K., et al. Risk of Bleeding with Single, Dual, or Triple Therapy with Warfarin, Aspirin, and Clopidogrel in Patients with Atrial Fibrillation. Arch. Intern. Med. 2010;170:1433–1441. doi: 10.1001/archinternmed.2010.271. - DOI - PubMed
-
- Gurwitz J.H., Field T.S., Harrold L.R., Rothschild J., Debellis K., Seger A.C., Cadoret C., Fish L.S., Garber L., Kelleher M., et al. Incidence and Preventability of Adverse Drug Events among Older Persons in the Ambulatory Setting. JAMA. 2003;289:1107–1116. doi: 10.1001/jama.289.9.1107. - DOI - PubMed
LinkOut - more resources
Full Text Sources
