

Deformity Reconstruction Surgery for Tibial Hemimelia
- PMID: 34072809
- PMCID: PMC8229975
- DOI: 10.3390/children8060461
Deformity Reconstruction Surgery for Tibial Hemimelia
Abstract
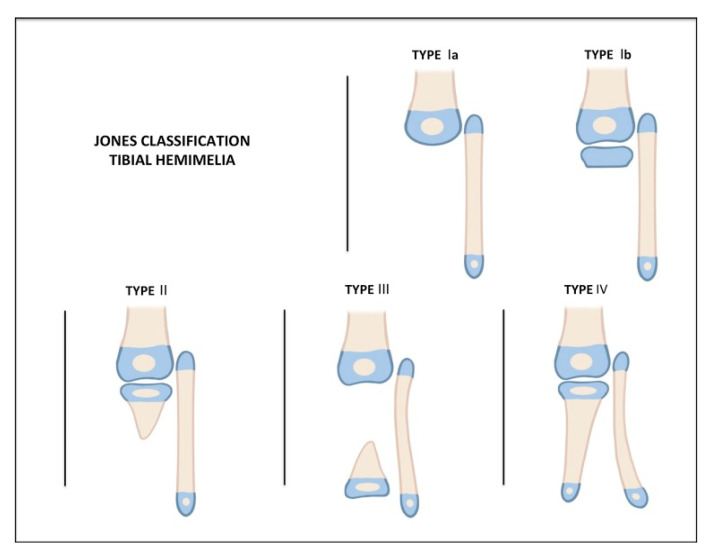
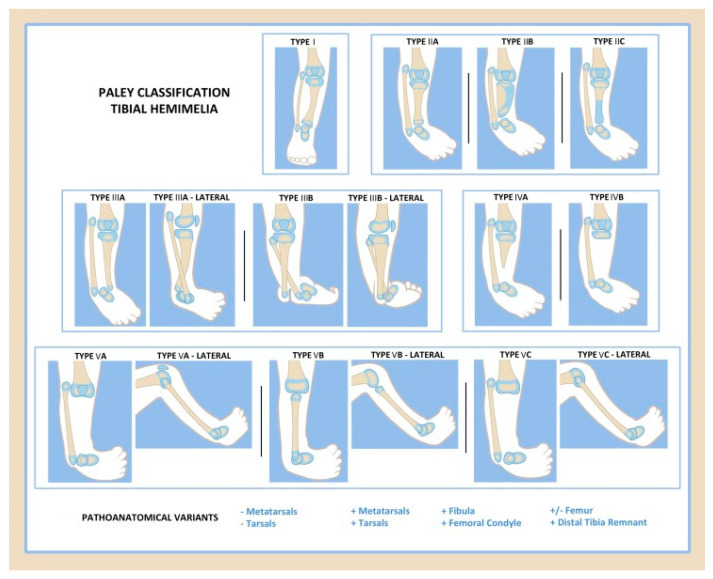
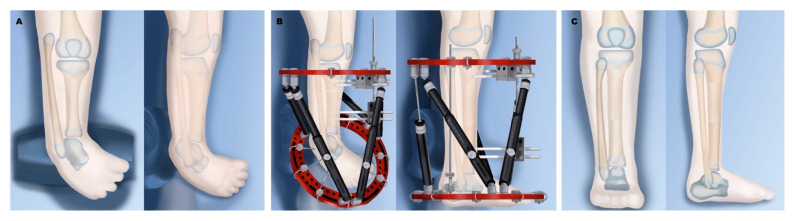
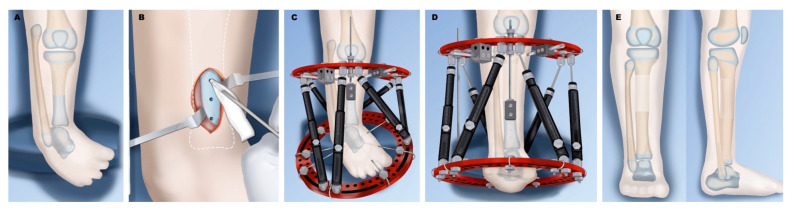
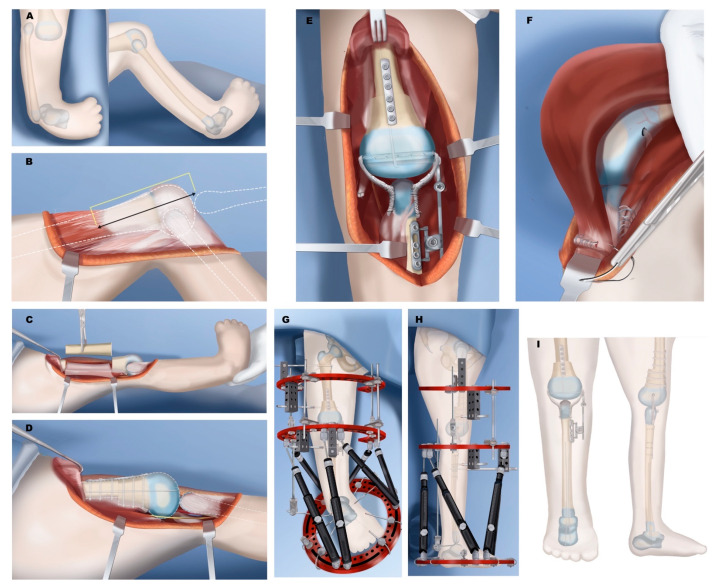
Tibial hemimelia is a rare congenital deficiency with a wide spectrum of pathology and deformity. This paper aims to give a comprehensive review of tibial hemimelia, with a concise summary of the history, pathology, and clinical findings of tibial hemimelia, while providing treatment recommendations and a review of the current literature. Classifications and surgical treatments are discussed, including amputation, limb reconstruction, and lengthening. Type-specific treatments are also discussed, including staged distraction correction of joint contractures of knee and ankle, Weber patelloplasty, fibular centralization, knee and ankle arthrodesis, implantable articulated distractors, and the role of femoral shortening. Amputation is a simpler and easier solution for many patients; however, reconstruction options continue to evolve, improve, and provide better functional outcomes in many cases. Factors favoring surgical reconstruction include the presence of a knee joint/proximal tibia, and the presence of a patella and quadriceps mechanism.
Keywords: Paley classification; absence of tibia; fibula centralization; patelloplasty; tibial aplasia; tibial deficiency; tibial hemimelia; treatment.
Conflict of interest statement
The authors declare no relevant conflict of interest.
Figures


References
-
- Brown F.W. The Brown Operation for Total Hemimelia Tibia. In: Aitken G.T., editor. Selected Lower-Limb Anomalies: Surgical and Prosthetics Management: A Symposium Held in Washington. The National Academies Press; Washington, DC, USA: 1971.
-
- Otto A.W. Monstrorum sexcentorum descriptio anatomica. Vratislaviae (Breslau): Sumptibus Ferdinandi Hirt, 1841. Print.
-
- Billroth T. Ueber einige durch Knochendefecte bedingte Krümmungen des Fusses. Arch Klin. Chir. 1861;1:252–268.
-
- Dankmeijer J. Congenital absence of the tibia. Anat. Rec. 1935;62:179194. doi: 10.1002/ar.1090620205. - DOI
Publication types
LinkOut - more resources
Full Text Sources
