

A Fair Assessment of Evaluation Tools for the Murine Microbead Occlusion Model of Glaucoma
- PMID: 34073191
- PMCID: PMC8199180
- DOI: 10.3390/ijms22115633
A Fair Assessment of Evaluation Tools for the Murine Microbead Occlusion Model of Glaucoma
Abstract
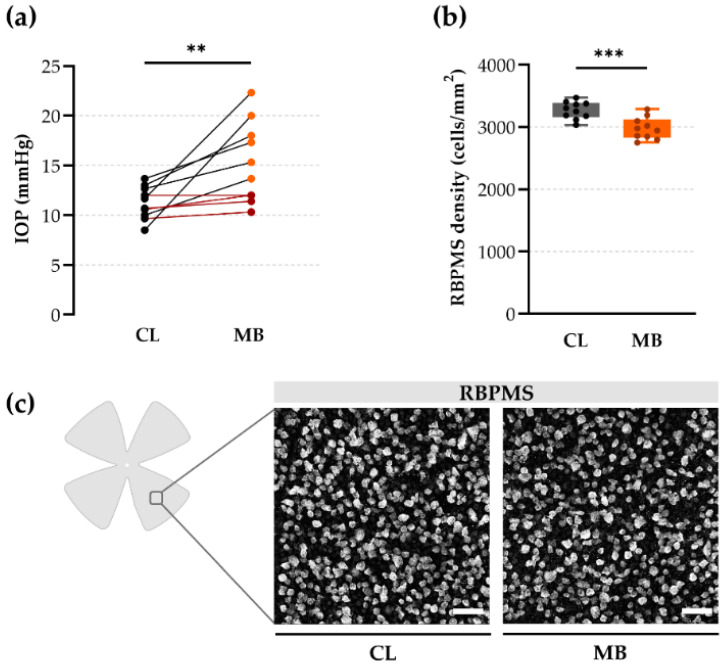
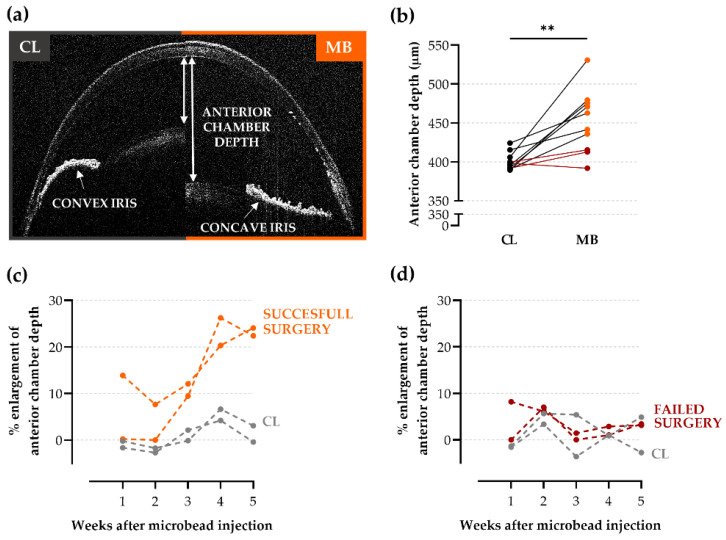
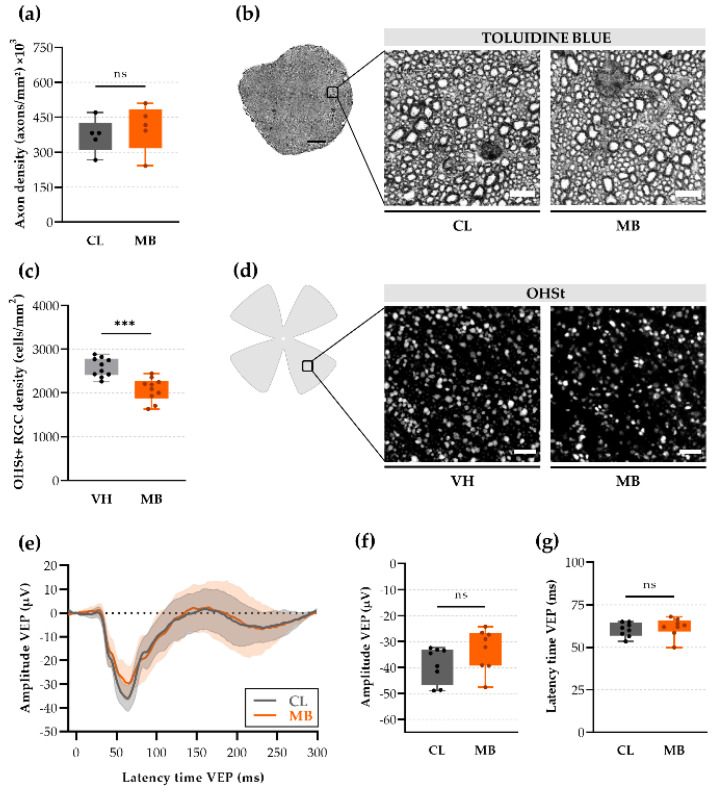
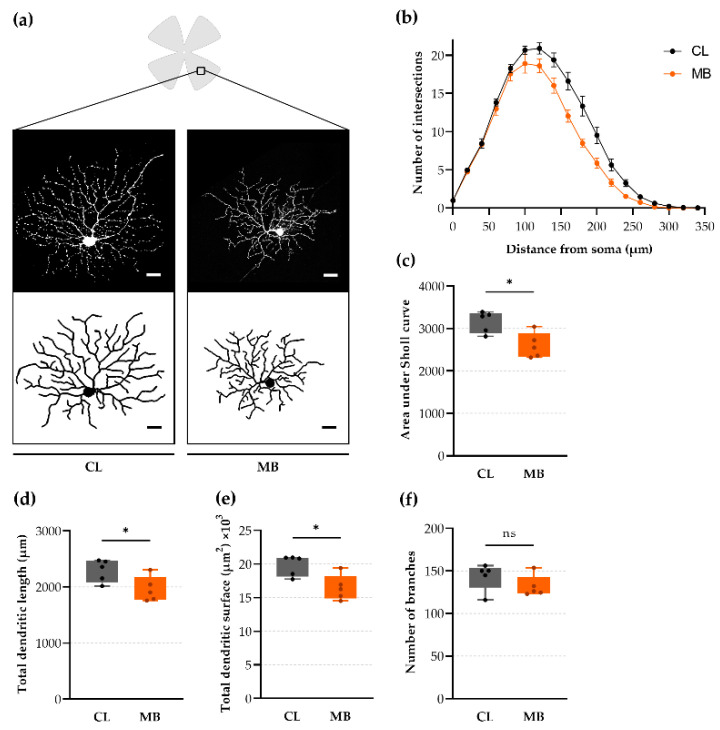
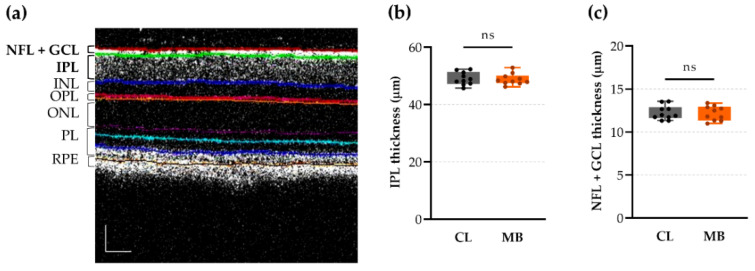
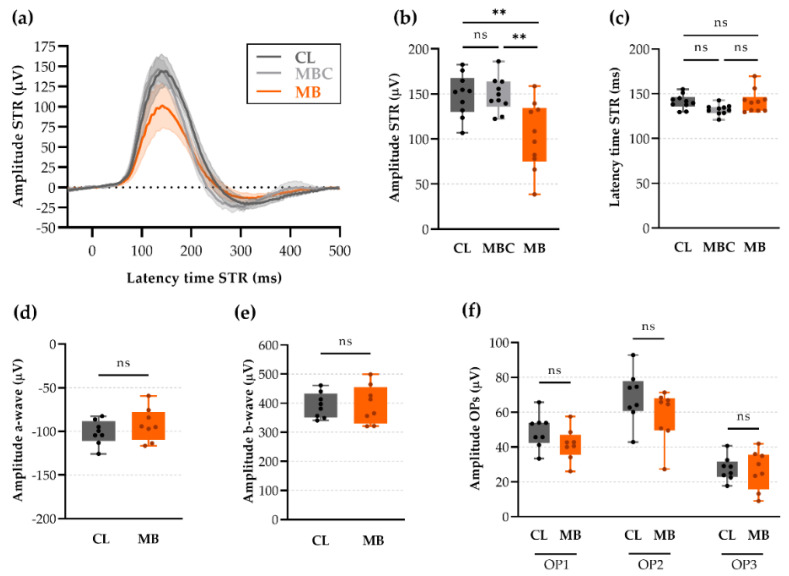
Despite being one of the most studied eye diseases, clinical translation of glaucoma research is hampered, at least in part, by the lack of validated preclinical models and readouts. The most popular experimental glaucoma model is the murine microbead occlusion model, yet the observed mild phenotype, mixed success rate, and weak reproducibility urge for an expansion of available readout tools. For this purpose, we evaluated various measures that reflect early onset glaucomatous changes in the murine microbead occlusion model. Anterior chamber depth measurements and scotopic threshold response recordings were identified as an outstanding set of tools to assess the model's success rate and to chart glaucomatous damage (or neuroprotection in future studies), respectively. Both are easy-to-measure, in vivo tools with a fast acquisition time and high translatability to the clinic and can be used, whenever judged beneficial, in combination with the more conventional measures in present-day glaucoma research (i.e., intraocular pressure measurements and post-mortem histological analyses). Furthermore, we highlighted the use of dendritic arbor analysis as an alternative histological readout for retinal ganglion cell density counts.
Keywords: anterior chamber depth; dendritic retraction; electroretinography; glaucoma; microbead occlusion model; neurodegeneration; ocular hypertension; optical coherence tomography; retinal ganglion cells; scotopic threshold response.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Comparative analysis of retinal ganglion cell damage in three glaucomatous rat models.Exp Eye Res. 2018 Jul;172:112-122. doi: 10.1016/j.exer.2018.03.019. Epub 2018 Mar 30. Exp Eye Res. 2018. PMID: 29605491
-
A Magnetic Microbead Occlusion Model to Induce Ocular Hypertension-Dependent Glaucoma in Mice.J Vis Exp. 2016 Mar 23;(109):e53731. doi: 10.3791/53731. J Vis Exp. 2016. PMID: 27077732 Free PMC article.
-
Microbead models in glaucoma.Exp Eye Res. 2015 Dec;141:9-14. doi: 10.1016/j.exer.2015.06.020. Epub 2015 Jun 24. Exp Eye Res. 2015. PMID: 26116904 Review.
-
Upregulation of the endothelin A (ETA) receptor and its association with neurodegeneration in a rodent model of glaucoma.BMC Neurosci. 2017 Mar 1;18(1):27. doi: 10.1186/s12868-017-0346-3. BMC Neurosci. 2017. PMID: 28249604 Free PMC article.
-
[The use of mice in glaucoma research --to clarify the mechanism of intraocular pressure regulation and retinal ganglion cell damage].Nippon Ganka Gakkai Zasshi. 2010 Mar;114(3):217-46; discussion 247. Nippon Ganka Gakkai Zasshi. 2010. PMID: 20387537 Review. Japanese.
Cited by
-
A deep phenotyping study in mouse and iPSC models to understand the role of oligodendroglia in optic neuropathy in Wolfram syndrome.Acta Neuropathol Commun. 2024 Aug 28;12(1):140. doi: 10.1186/s40478-024-01851-7. Acta Neuropathol Commun. 2024. PMID: 39198924 Free PMC article.
-
A new microfluidic model to study dendritic remodeling and mitochondrial dynamics during axonal regeneration of adult zebrafish retinal neurons.Front Mol Neurosci. 2023 Jun 15;16:1196504. doi: 10.3389/fnmol.2023.1196504. eCollection 2023. Front Mol Neurosci. 2023. PMID: 37396787 Free PMC article.
-
Chronic Chemogenetic Activation of the Superior Colliculus in Glaucomatous Mice: Local and Retrograde Molecular Signature.Cells. 2022 May 29;11(11):1784. doi: 10.3390/cells11111784. Cells. 2022. PMID: 35681479 Free PMC article.
-
Retinal Ganglion Cells: Global Number, Density and Vulnerability to Glaucomatous Injury in Common Laboratory Mice.Cells. 2022 Aug 29;11(17):2689. doi: 10.3390/cells11172689. Cells. 2022. PMID: 36078097 Free PMC article.
References
-
- Frankfort B.J., Khan A.K., Tse D.Y., Chung I., Pang J.-J., Yang Z., Gross R.L., Wu S.M. Elevated Intraocular Pressure Causes Inner Retinal Dysfunction Before Cell Loss in a Mouse Model of Experimental Glaucoma. Investig. Opthalmol. Vis. Sci. 2013;54:762. doi: 10.1167/iovs.12-10581. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
