

Occlusion of the Superior Mesenteric Artery in Rats Reversed by Collateral Pathways Activation: Gastric Pentadecapeptide BPC 157 Therapy Counteracts Multiple Organ Dysfunction Syndrome; Intracranial, Portal, and Caval Hypertension; and Aortal Hypotension
- PMID: 34073625
- PMCID: PMC8229949
- DOI: 10.3390/biomedicines9060609
Occlusion of the Superior Mesenteric Artery in Rats Reversed by Collateral Pathways Activation: Gastric Pentadecapeptide BPC 157 Therapy Counteracts Multiple Organ Dysfunction Syndrome; Intracranial, Portal, and Caval Hypertension; and Aortal Hypotension
Abstract
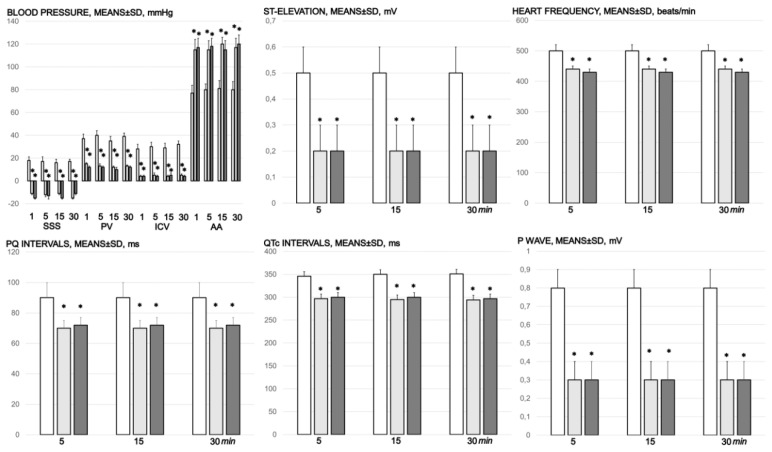
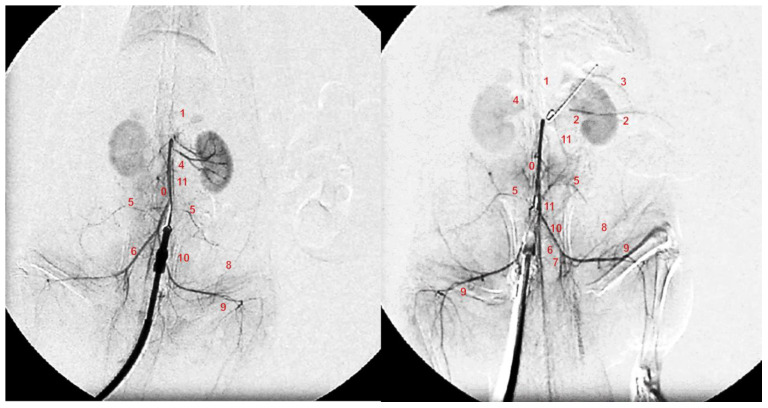
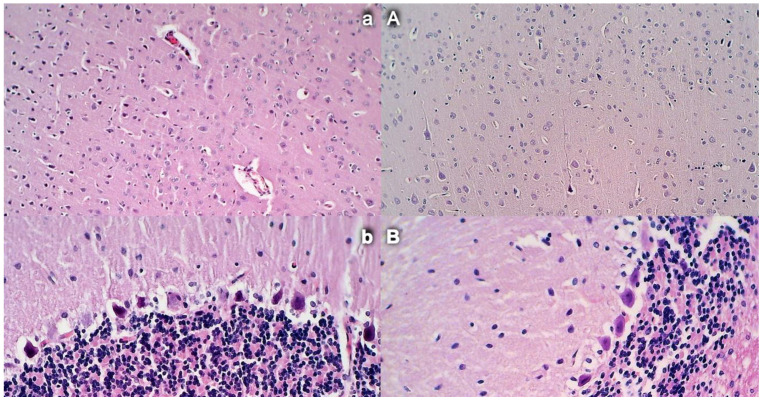
Gastric pentadecapeptide BPC 157 therapy counteracts multiple organ dysfunction syndrome in rats, which have permanent occlusion of the superior mesenteric artery close to the abdominal aorta. Previously, when confronted with major vessel occlusion, its effect would rapidly activate collateral vessel pathways and resolve major venous occlusion syndromes (Pringle maneuver ischemia, reperfusion, Budd-Chiari syndrome) in rats. This would overwhelm superior mesenteric artery permanent occlusion, and result in local, peripheral, and central disturbances. Methods: Assessments, for 30 min (gross recording, angiography, ECG, pressure, microscopy, biochemistry, and oxidative stress), included the portal hypertension, caval hypertension, and aortal hypotension, and centrally, the superior sagittal sinus hypertension; systemic arterial and venous thrombosis; ECG disturbances; MDA-tissue increase; and multiple organ lesions and disturbances, including the heart, lung, liver, kidney, and gastrointestinal tract, in particular, as well as brain (cortex (cerebral, cerebellar), hypothalamus/thalamus, hippocampus). BPC 157 therapy (/kg, abdominal bath) (10 µg, 10 ng) was given for a 1-min ligation time. Results: BPC 157 rapidly recruits collateral vessels (inferior anterior pancreaticoduodenal artery and inferior mesenteric artery) that circumvent occlusion and ascertains blood flow distant from the occlusion in the superior mesenteric artery. Portal and caval hypertension, aortal hypotension, and, centrally, superior sagittal sinus hypertension were attenuated or eliminated, and ECG disturbances markedly mitigated. BPC 157 therapy almost annihilated venous and arterial thrombosis. Multiple organ lesions and disturbances (i.e., heart, lung, liver, and gastrointestinal tract, in particular, as well as brain) were largely attenuated. Conclusions: Rats with superior mesenteric artery occlusion may additionally undergo BPC 157 therapy as full counteraction of vascular occlusion-induced multiple organ dysfunction syndrome.
Keywords: BPC 157; rats; superior mesenteric artery occlusion; vascular recruitment.
Conflict of interest statement
The authors declare that there are no conflict of interest.
Figures












Similar articles
-
Complex Syndrome of the Complete Occlusion of the End of the Superior Mesenteric Vein, Opposed with the Stable Gastric Pentadecapeptide BPC 157 in Rats.Biomedicines. 2021 Aug 17;9(8):1029. doi: 10.3390/biomedicines9081029. Biomedicines. 2021. PMID: 34440233 Free PMC article.
-
Occluded Superior Mesenteric Artery and Vein. Therapy with the Stable Gastric Pentadecapeptide BPC 157.Biomedicines. 2021 Jul 8;9(7):792. doi: 10.3390/biomedicines9070792. Biomedicines. 2021. PMID: 34356860 Free PMC article.
-
BPC 157 Therapy and the Permanent Occlusion of the Superior Sagittal Sinus in Rat: Vascular Recruitment.Biomedicines. 2021 Jun 28;9(7):744. doi: 10.3390/biomedicines9070744. Biomedicines. 2021. PMID: 34203464 Free PMC article.
-
New studies with stable gastric pentadecapeptide protecting gastrointestinal tract. significance of counteraction of vascular and multiorgan failure of occlusion/occlusion-like syndrome in cytoprotection/organoprotection.Inflammopharmacology. 2024 Oct;32(5):3119-3161. doi: 10.1007/s10787-024-01499-8. Epub 2024 Jul 9. Inflammopharmacology. 2024. PMID: 38980576 Review.
-
Stable Gastric Pentadecapeptide BPC 157 May Recover Brain-Gut Axis and Gut-Brain Axis Function.Pharmaceuticals (Basel). 2023 Apr 30;16(5):676. doi: 10.3390/ph16050676. Pharmaceuticals (Basel). 2023. PMID: 37242459 Free PMC article. Review.
Cited by
-
Stomach perforation-induced general occlusion/occlusion-like syndrome and stable gastric pentadecapeptide BPC 157 therapy effect.World J Gastroenterol. 2023 Jul 21;29(27):4289-4316. doi: 10.3748/wjg.v29.i27.4289. World J Gastroenterol. 2023. PMID: 37545637 Free PMC article.
-
Robert's Intragastric Alcohol-Induced Gastric Lesion Model as an Escalated General Peripheral and Central Syndrome, Counteracted by the Stable Gastric Pentadecapeptide BPC 157.Biomedicines. 2021 Sep 23;9(10):1300. doi: 10.3390/biomedicines9101300. Biomedicines. 2021. PMID: 34680419 Free PMC article.
-
Acute Compartment Syndrome and Intra-Abdominal Hypertension, Decompression, Current Pharmacotherapy, and Stable Gastric Pentadecapeptide BPC 157 Solution.Pharmaceuticals (Basel). 2025 Jun 10;18(6):866. doi: 10.3390/ph18060866. Pharmaceuticals (Basel). 2025. PMID: 40573261 Free PMC article. Review.
-
Complex Syndrome of the Complete Occlusion of the End of the Superior Mesenteric Vein, Opposed with the Stable Gastric Pentadecapeptide BPC 157 in Rats.Biomedicines. 2021 Aug 17;9(8):1029. doi: 10.3390/biomedicines9081029. Biomedicines. 2021. PMID: 34440233 Free PMC article.
-
Innate Vascular Failure by Application of Neuroleptics, Amphetamine, and Domperidone Rapidly Induced Severe Occlusion/Occlusion-like Syndromes in Rats and Stable Gastric Pentadecapeptide BPC 157 as Therapy.Pharmaceuticals (Basel). 2023 May 25;16(6):788. doi: 10.3390/ph16060788. Pharmaceuticals (Basel). 2023. PMID: 37375736 Free PMC article.
References
-
- Sikiric P., Petek M., Rucman R., Seiwerth S., Grabarevic Z., Rotkvic I., Turkovic B., Jagic V., Mildner B., Duvnjak M., et al. A new gastric juice peptide, BPC. An overview of the stomach-stress-organoprotection hypothesis and beneficial effects of BPC. J. Physiol. Paris. 1993;87:313–327. doi: 10.1016/0928-4257(93)90038-U. - DOI - PubMed
-
- Sikiric P., Seiwerth S., Brcic L., Blagaic A.B., Zoricic I., Sever M., Klicek R., Radic B., Keller N., Sipos K., et al. Stable gastric pentadecapeptide BPC 157 in trials for inflammatory bowel disease (PL-10, PLD-116, PL 14736, Pliva, Croatia). Full and distended stomach, and vascular response. Inflammopharmacology. 2006;14:214–221. doi: 10.1007/s10787-006-1531-7. - DOI - PubMed
-
- Sikiric P., Seiwerth S., Brcic L., Sever M., Klicek R., Radic B., Drmic D., Ilic S., Kolenc D. Revised Robert’s cytoprotection and adaptive cytoprotection and stable gastric pentadecapeptide BPC 157. Possible significance and implications for novel mediator. Curr. Pharm. Des. 2010;16:1224–1234. doi: 10.2174/138161210790945977. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
