

Identifying individual hospital levels of maternal care using administrative data
- PMID: 34074286
- PMCID: PMC8171026
- DOI: 10.1186/s12913-021-06516-y
Identifying individual hospital levels of maternal care using administrative data
Abstract
Background: The goal of regionalized perinatal care, specifically levels of maternal care, is to improve maternal outcomes through risk-appropriate obstetric care. Studies of levels of maternal care are limited by current approaches to identify a hospital's level of care, often relying on hospital self-reported data, which is expensive and challenging to collect and validate. The study objective was to develop an empiric approach to determine a hospital's level of maternal care using administrative data reflective of the patient care provided and apply this approach to describe the levels of maternal care available over time.
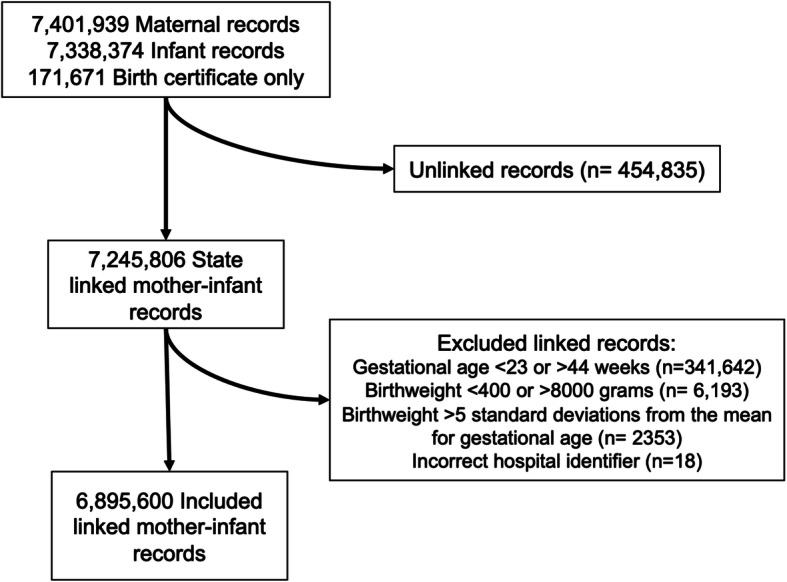
Methods: Retrospective cohort study of mother-infant dyads who delivered in California, Missouri, and Pennsylvania hospitals from 2000 to 2009. Linked mother-infant administrative records with an infant born at 24-44 weeks' gestation and a birth weight of 400-8000 g were included. Using the American College of Obstetricians and Gynecologists and the Society for Maternal Fetal Medicine descriptions of levels of maternal care, four levels were classified based on the appropriate location of care for patients with specific medical or pregnancy conditions. Individual hospitals were assigned a level of maternal care annually based on the volume of patients who delivered reflective of the four classified levels as determined by International Classification of Diseases and Current Procedural Terminology.
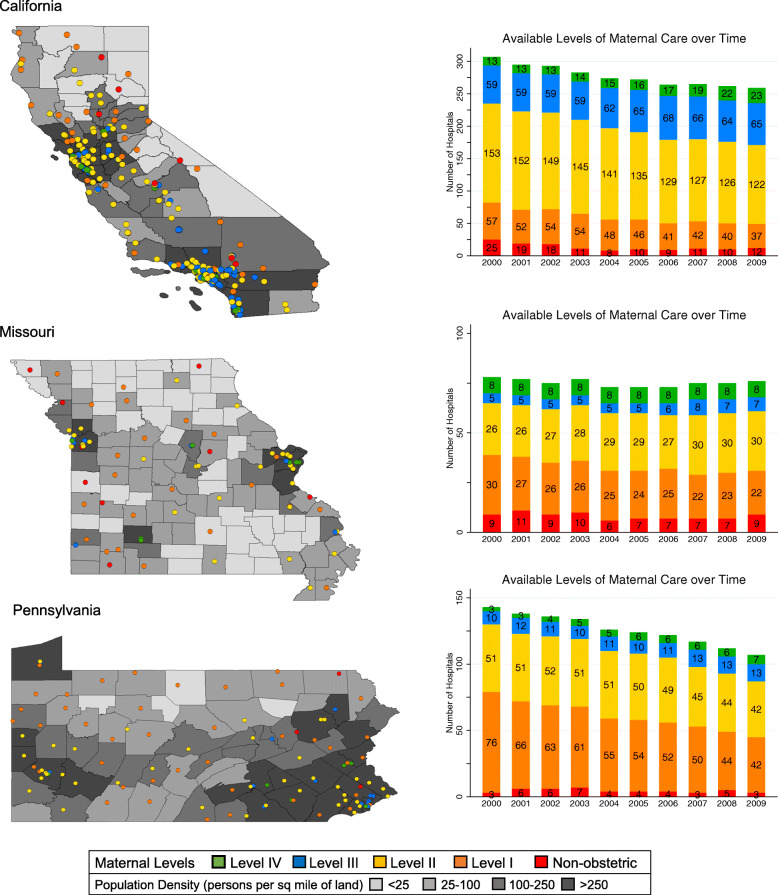
Results: Based on the included 6,895,000 mother-infant dyads, the obstetric hospital levels of maternal care I, II, III and IV were identified. High-risk patients more frequently delivered in hospitals with higher level maternal care, accounting for 8.9, 10.9, 13.8, and 16.9% of deliveries in level I, II, III and IV hospitals, respectively. The total number of obstetric hospitals decreased over the study period, while the proportion of hospitals with high-level (level III or IV) maternal care increased. High-level hospitals were located in more densely populated areas.
Conclusion: Identification of the level of maternal care, independent of hospital self-reported variables, is feasible using administrative data. This empiric approach, which accounts for changes in hospitals over time, is a valuable framework for perinatal researchers and other stakeholders to inexpensively identify measurable benefits of levels of maternal care and characterize where specific patient populations receive care.
Keywords: Perinatal care; Regionalization; Risk-appropriate.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The differential impact of delivery hospital on the outcomes of premature infants.Pediatrics. 2012 Aug;130(2):270-8. doi: 10.1542/peds.2011-2820. Epub 2012 Jul 9. Pediatrics. 2012. PMID: 22778301 Free PMC article.
-
The effect of hospital acuity on severe maternal morbidity in high-risk patients.Am J Obstet Gynecol. 2018 Jul;219(1):111.e1-111.e7. doi: 10.1016/j.ajog.2018.04.015. Epub 2018 Apr 16. Am J Obstet Gynecol. 2018. PMID: 29673571
-
Operationalizing risk-appropriate perinatal care in a rural US State: directions for policy and practice.BMC Health Serv Res. 2023 Jun 8;23(1):601. doi: 10.1186/s12913-023-09552-y. BMC Health Serv Res. 2023. PMID: 37291539 Free PMC article.
-
Obstetric Care Consensus #9: Levels of Maternal Care: (Replaces Obstetric Care Consensus Number 2, February 2015).Am J Obstet Gynecol. 2019 Dec;221(6):B19-B30. doi: 10.1016/j.ajog.2019.05.046. Epub 2019 Jul 25. Am J Obstet Gynecol. 2019. PMID: 31351999
-
Obstetrical complications associated with abnormal maternal serum markers analytes.J Obstet Gynaecol Can. 2008 Oct;30(10):918-932. doi: 10.1016/S1701-2163(16)32973-5. J Obstet Gynaecol Can. 2008. PMID: 19038077 Review. English, French.
Cited by
-
Factors associated with antepartum pilgrimage at a reference maternity hospital in Ceará.Rev Esc Enferm USP. 2024 Apr 12;58:e20230012. doi: 10.1590/1980-220X-REEUSP-2023-0012en. eCollection 2024. Rev Esc Enferm USP. 2024. PMID: 38634686 Free PMC article.
-
Patients in Iowa Counties Lacking Hospitals With Labor and Delivery Services Disproportionately Receive Care at Level III Maternal Care Hospitals When Undergoing Cesarean Delivery: A Retrospective Longitudinal Study.Cureus. 2022 Oct 25;14(10):e30683. doi: 10.7759/cureus.30683. eCollection 2022 Oct. Cureus. 2022. PMID: 36439612 Free PMC article.
-
Busy day effect on the use of obstetrical interventions and epidural analgesia during labour: a cross-sectional register study of 601 247 deliveries.BMC Pregnancy Childbirth. 2022 Jun 13;22(1):481. doi: 10.1186/s12884-022-04798-6. BMC Pregnancy Childbirth. 2022. PMID: 35698049 Free PMC article.
-
Validation of a measure of hospital maternal level of care for the United States.BMC Health Serv Res. 2024 Mar 6;24(1):286. doi: 10.1186/s12913-024-10754-1. BMC Health Serv Res. 2024. PMID: 38443900 Free PMC article.
References
-
- Centers for Disease Control and Prevention. Severe Maternal Morbidity in the United States: Centers for Disease Control and Prevention; 2017. Available from: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/severematern... Accessed 20 Jan 2020.
-
- Institute of Medicine. Committee on the Future of Emergency Care in the United States Health. Board on Health Care Services . Emergency medical services: at the crossroads. Washington: National Academies Press; 2006.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
