

The cytokine storms of COVID-19, H1N1 influenza, CRS and MAS compared. Can one sized treatment fit all?
- PMID: 34074585
- PMCID: PMC8149193
- DOI: 10.1016/j.cyto.2021.155593
The cytokine storms of COVID-19, H1N1 influenza, CRS and MAS compared. Can one sized treatment fit all?
Abstract
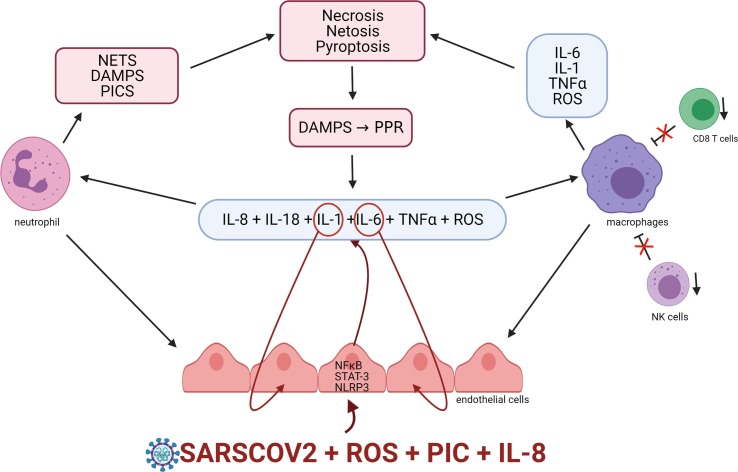
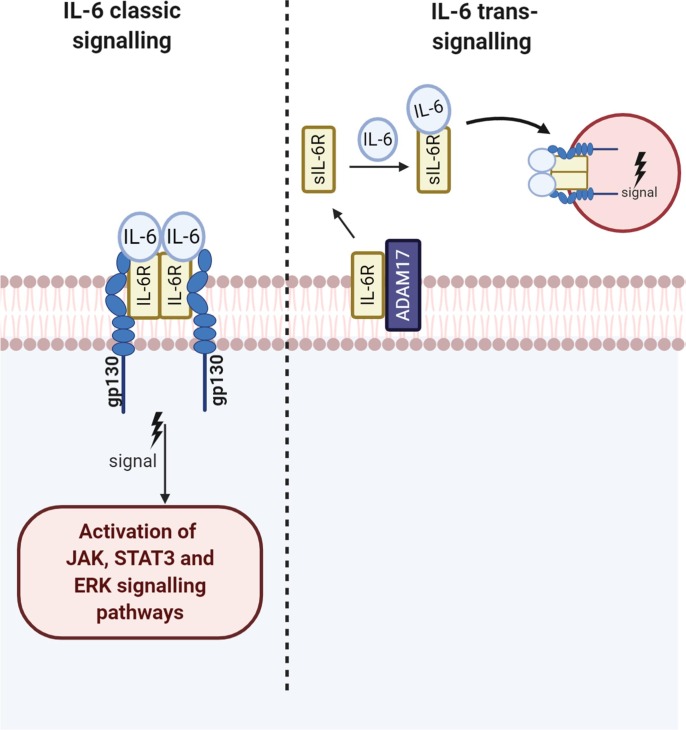
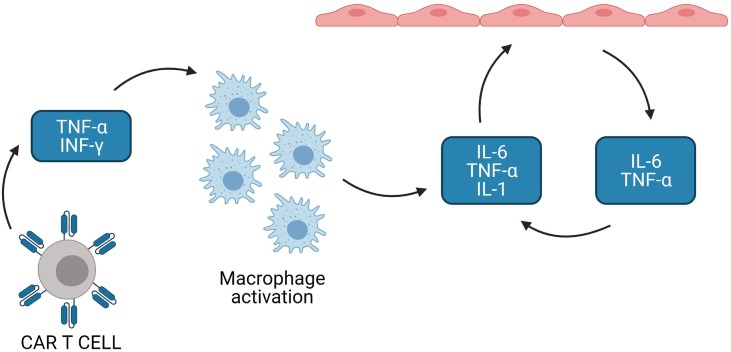
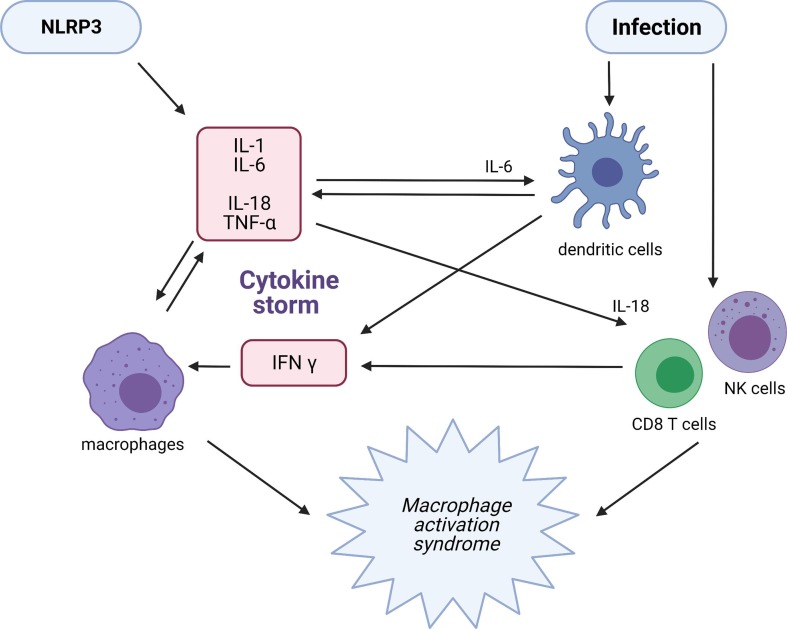
An analysis of published data appertaining to the cytokine storms of COVID-19, H1N1 influenza, cytokine release syndrome (CRS), and macrophage activation syndrome (MAS) reveals many common immunological and biochemical abnormalities. These include evidence of a hyperactive coagulation system with elevated D-dimer and ferritin levels, disseminated intravascular coagulopathy (DIC) and microthrombi coupled with an activated and highly permeable vascular endothelium. Common immune abnormalities include progressive hypercytokinemia with elevated levels of TNF-α, interleukin (IL)-6, and IL-1β, proinflammatory chemokines, activated macrophages and increased levels of nuclear factor kappa beta (NFκB). Inflammasome activation and release of damage associated molecular patterns (DAMPs) is common to COVID-19, H1N1, and MAS but does not appear to be a feature of CRS. Elevated levels of IL-18 are detected in patients with COVID-19 and MAS but have not been reported in patients with H1N1 influenza and CRS. Elevated interferon-γ is common to H1N1, MAS, and CRS but levels of this molecule appear to be depressed in patients with COVID-19. CD4+ T, CD8+ and NK lymphocytes are involved in the pathophysiology of CRS, MAS, and possibly H1N1 but are reduced in number and dysfunctional in COVID-19. Additional elements underpinning the pathophysiology of cytokine storms include Inflammasome activity and DAMPs. Treatment with anakinra may theoretically offer an avenue to positively manipulate the range of biochemical and immune abnormalities reported in COVID-19 and thought to underpin the pathophysiology of cytokine storms beyond those manipulated via the use of, canakinumab, Jak inhibitors or tocilizumab. Thus, despite the relative success of tocilizumab in reducing mortality in COVID-19 patients already on dexamethasone and promising results with Baricitinib, the combination of anakinra in combination with dexamethasone offers the theoretical prospect of further improvements in patient survival. However, there is currently an absence of trial of evidence in favour or contravening this proposition. Accordingly, a large well powered blinded prospective randomised controlled trial (RCT) to test this hypothesis is recommended.
Keywords: COVID-19; Cytokine storm; Immune; Inflammation; Interleukin-1; Interleukin-6.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Moore B.J.B., June C.H. Cytokine release syndrome in severe COVID-19. Science. 2020:eabb8925. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
