Association between confirmed congenital Zika infection at birth and outcomes up to 3 years of life
- PMID: 34075035
- PMCID: PMC8169933
- DOI: 10.1038/s41467-021-23468-3
Association between confirmed congenital Zika infection at birth and outcomes up to 3 years of life
Abstract
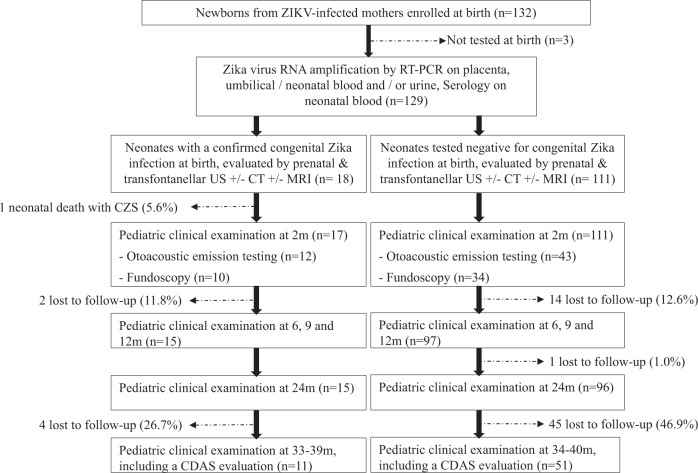
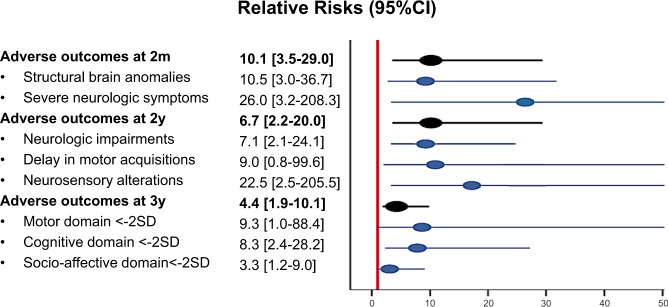
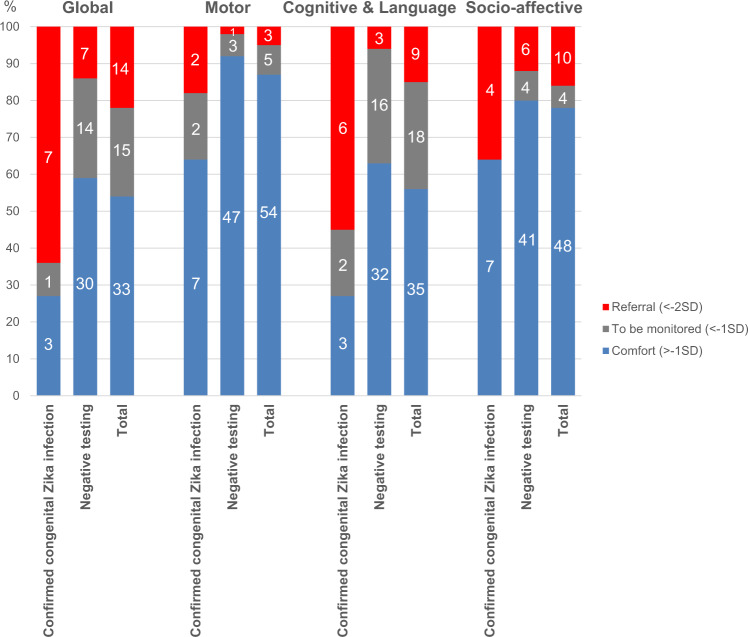
Little is known about the long-term neurological development of children diagnosed with congenital Zika infection at birth. Here, we report the imaging and clinical outcomes up to three years of life of a cohort of 129 children exposed to Zika virus in utero. Eighteen of them (14%) had a laboratory confirmed congenital Zika infection at birth. Infected neonates have a higher risk of adverse neonatal and early infantile outcomes (death, structural brain anomalies or neurologic symptoms) than those who tested negative: 8/18 (44%) vs 4/111 (4%), aRR 10.1 [3.5-29.0]. Neurological impairment, neurosensory alterations or delays in motor acquisition are more common in infants with a congenital Zika infection at birth: 6/15 (40%) vs 5/96 (5%), aRR 6.7 [2.2-20.0]. Finally, infected children also have an increased risk of subspecialty referral for suspected neurodevelopmental delay by three years of life: 7/11 (64%) vs 7/51 (14%), aRR 4.4 [1.9-10.1]. Infected infants without structural brain anomalies also appear to have an increased risk, although to a lesser extent, of neurological abnormalities. It seems paramount to offer systematic testing for congenital ZIKV infection in cases of in utero exposure and adapt counseling based on these results.
Conflict of interest statement
The authors declare no competing interests.
Figures